Department of Ophthalmology, Sydney Eye Hospital, 8 Macquarie Street, Sydney, 2000, Australia.
Discipline of Ophthalmology, The University of Sydney, Camperdown, Australia.
Int Ophthalmol. 2023 Aug;43(8):2763-2776. doi: 10.1007/s10792-023-02675-5. Epub 2023 Mar 13.
Neovascular glaucoma (NVG) is a sight-threatening condition that is often refractory to treatment. Current management principles are yet to be standardized due to lack of evidence. We studied the interventions used to treat NVG at Sydney Eye Hospital (SEH) and the two-year surgical outcomes.
We performed a retrospective audit of 67 eyes of 58 patients with NVG from January 1, 2013, to December 31, 2018. Intraocular pressure (IOP), best-corrected visual acuity (BCVA), number of medications, repeat surgery, recurrent neovascularization, loss of light perception and pain were studied.
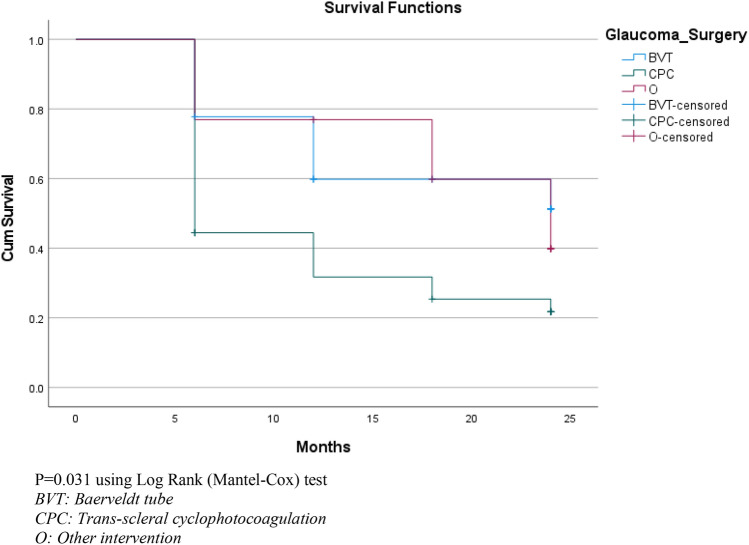
The average age of the cohort was 59.67 years (SD 14.22). The most common etiologies were proliferative diabetic retinopathy (35 eyes; 52.2%), central retinal vein occlusion (18 eyes; 26.9%) and ocular ischemic syndrome (7 eyes; 10.4%). 70.1% of eyes (47) received vascular endothelial growth factor injections (VEGFI), 41.8% (28 eyes) received pan-retinal photocoagulation (PRP) and 37.3% (25 eyes) received both prior to or within the first week of presentation to SEH. The most common initial surgical interventions were trans-scleral cyclophotocoagulation (TSCPC) (36 eyes; 53.7%) and Baerveldt tube insertion (18 eyes; 26.9%). 62.7% of eyes (42 eyes) failed (IOP > 21 or < 6 mmHg for two consecutive reviews, further IOP-lowering surgery or loss of light perception) during follow-up. Initial TSCPC failed in 75.0% (27/36 eyes) compared with 44.4% (8/18 eyes) after Baerveldt tube insertion.
Our study reinforces the refractory nature of NVG, often despite intensive treatment and surgery. Improvements in patient outcomes may be achieved with earlier consideration of VEGFI and PRP. This study identifies the limitations of surgical interventions for NVG and highlights the need for a standardized management approach.
新生血管性青光眼(NVG)是一种威胁视力的疾病,通常对治疗有抗性。由于缺乏证据,目前的管理原则尚未标准化。我们研究了 2013 年 1 月 1 日至 2018 年 12 月 31 日期间在悉尼眼科医院(SEH)治疗 NVG 所使用的干预措施以及两年的手术结果。
我们对 2013 年 1 月 1 日至 2018 年 12 月 31 日期间因 NVG 在 SEH 接受治疗的 58 例 67 只眼的患者进行了回顾性审计。研究了眼压(IOP)、最佳矫正视力(BCVA)、药物数量、重复手术、新生血管复发、光感丧失和疼痛。
该队列的平均年龄为 59.67 岁(SD 14.22)。最常见的病因是增生性糖尿病视网膜病变(35 只眼;52.2%)、视网膜中央静脉阻塞(18 只眼;26.9%)和眼缺血综合征(7 只眼;10.4%)。70.1%(47 只眼)的患者接受了血管内皮生长因子注射(VEGFI),41.8%(28 只眼)接受了全视网膜光凝(PRP),37.3%(25 只眼)在 SEH 就诊的第一周内或之前接受了上述治疗。最常见的初始手术干预措施是经巩膜睫状体光凝术(TSCPC)(36 只眼;53.7%)和 Baerveldt 管插入术(18 只眼;26.9%)。62.7%(42 只眼)的患者在随访过程中(IOP>21mmHg 或<6mmHg 连续两次复查,进一步降眼压手术或光感丧失)失败。初始 TSCPC 失败率为 75.0%(27/36 只眼),Baerveldt 管插入术后为 44.4%(8/18 只眼)。
我们的研究证实了 NVG 的难治性,尽管进行了强化治疗和手术。早期考虑 VEGFI 和 PRP 可能会改善患者的预后。本研究确定了 NVG 手术干预的局限性,并强调需要标准化的管理方法。