Department of Urology, Comprehensive Cancer Center, Medical University of Vienna, Vienna, Austria.
Department of Urology, The Jikei University School of Medicine, Tokyo.
Curr Opin Urol. 2023 Jul 1;33(4):258-268. doi: 10.1097/MOU.0000000000001097. Epub 2023 Apr 3.
Although lymph node dissection (LND) during radical nephroureterectomy (RNU) is recommended for high-risk nonmetastatic upper tract urothelial carcinoma (UTUC), adherence to guidelines remains insufficient in clinical practice. Therefore, this review aims to comprehensively summarize the current evidence regarding the diagnostic, prognostic, and therapeutic impact of LND during RNU in UTUC patients.
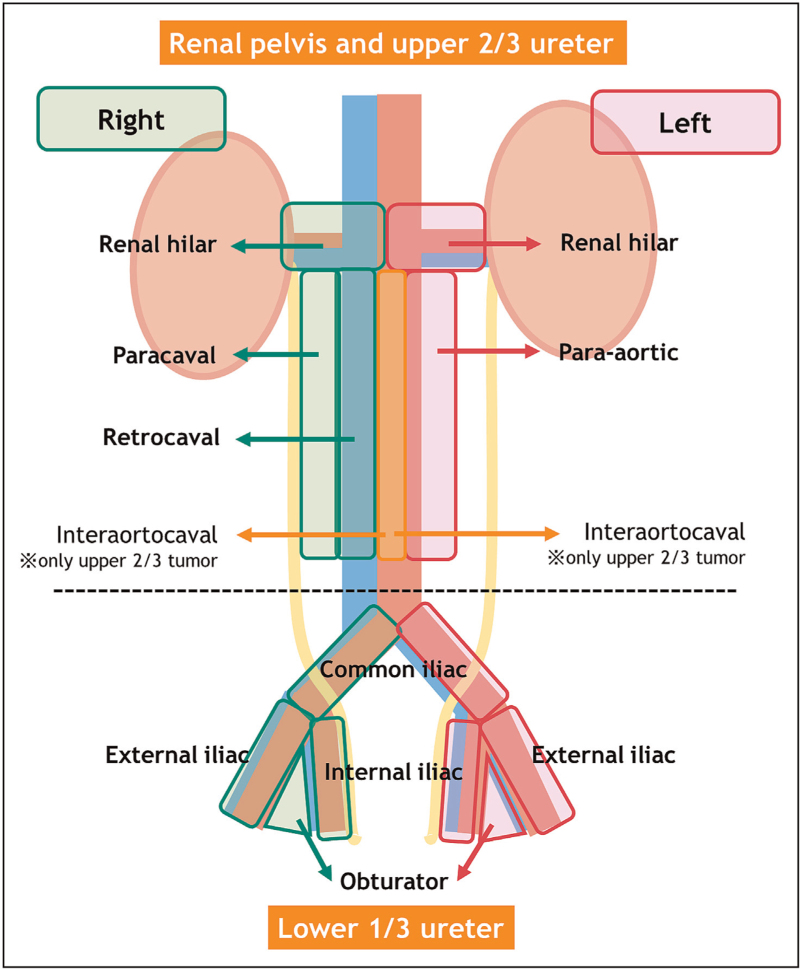
Clinical nodal staging using conventional CT scan has low sensitivity (25%) and diagnostic accuracy [area under the curve (AUC): 0.58] in UTUC, suggesting the importance of LND for obtaining accurate N-staging. Patients with pathological node-positive (pN+) disease have poor disease-free survival (DFS), cancer-specific survival (CSS), and overall survival (OS) compared with those with pN0. In addition, population-based studies showed that patients who underwent LND improved CSS and OS than those who did not, even in patients who received adjuvant systemic therapy. The number of lymph nodes removed has also been shown to be associated with improved CSS and OS, even in pT0 patients. Template-based LND should be performed as the extent of lymph node is more important than the number of lymph nodes. Robot-assisted RNU may facilitate performing a meticulous LND compared with a laparoscopic approach. Postoperative complications such as lymphatic and/or chylous leakage are increased but adequately manageable. However, the current evidence is not supported by high-quality studies.
Based on the published data, LND during RNU is a standard procedure for high-risk nonmetastatic UTUC, owing to its diagnostic, staging, prognostic, and, potentially, therapeutic benefits. Template-based LND should be offered to all patients who are planned for RNU for high-risk nonmetastatic UTUC. Patients with pN+ disease are optimal candidates for adjuvant systemic therapy. Robot-assisted RNU may facilitate meticulous LND compared with laparoscopic RNU.
虽然根治性肾输尿管切除术(RNU)时进行淋巴结清扫(LND)被推荐用于高危非转移性上尿路上皮癌(UTUC),但在临床实践中,对指南的遵循仍不充分。因此,本综述旨在全面总结当前关于 UTUC 患者 RNU 时 LND 的诊断、预后和治疗影响的证据。
在 UTUC 中,常规 CT 扫描进行临床淋巴结分期的敏感性(25%)和诊断准确性[曲线下面积(AUC):0.58]较低,提示 LND 对获得准确的 N 分期很重要。与 pN0 患者相比,病理淋巴结阳性(pN+)患者的无病生存(DFS)、癌症特异性生存(CSS)和总生存(OS)较差。此外,基于人群的研究表明,与未接受 LND 的患者相比,接受 LND 的患者 CSS 和 OS 得到改善,即使在接受辅助全身治疗的患者中也是如此。切除的淋巴结数量也与 CSS 和 OS 的改善相关,即使在 pT0 患者中也是如此。应进行基于模板的 LND,因为淋巴结的范围比淋巴结的数量更重要。与腹腔镜方法相比,机器人辅助 RNU 可能更有利于进行精细的 LND。术后并发症(如淋巴和/或乳糜漏)增加,但可充分管理。然而,目前的证据没有得到高质量研究的支持。
基于已发表的数据,由于 LND 具有诊断、分期、预后和潜在的治疗益处,因此在 RNU 时对高危非转移性 UTUC 进行 LND 是一种标准程序。对于计划进行高危非转移性 UTUC 的 RNU 的所有患者,应提供基于模板的 LND。pN+疾病患者是辅助全身治疗的最佳候选者。与腹腔镜 RNU 相比,机器人辅助 RNU 可能更有利于进行精细的 LND。