The Royal Marsden NHS Foundation Trust, London, United Kingdom.
Fondazione IRCCS Istituto Nazionale dei Tumori, Milan, Italy.
Clin Cancer Res. 2023 Sep 1;29(17):3352-3361. doi: 10.1158/1078-0432.CCR-22-3145.
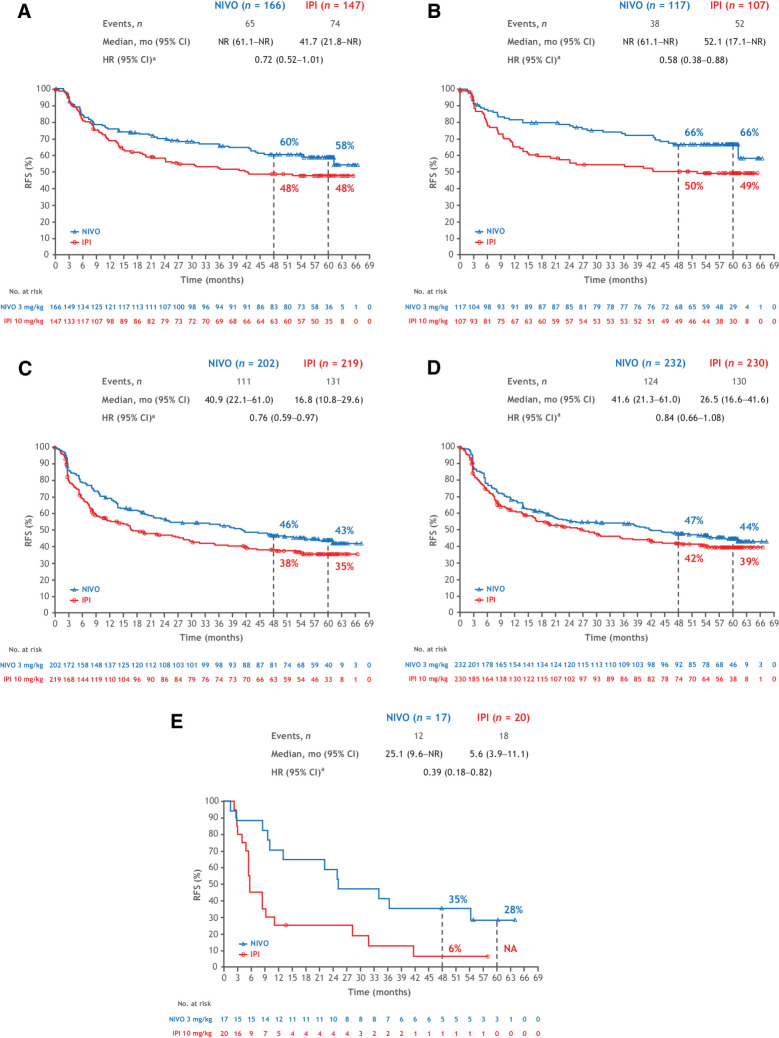
In the phase III CheckMate 238 study, adjuvant nivolumab significantly improved recurrence-free survival (RFS) and distant metastasis-free survival versus ipilimumab in patients with resected stage IIIB-C or stage IV melanoma, with benefit sustained at 4 years. We report updated 5-year efficacy and biomarker findings.
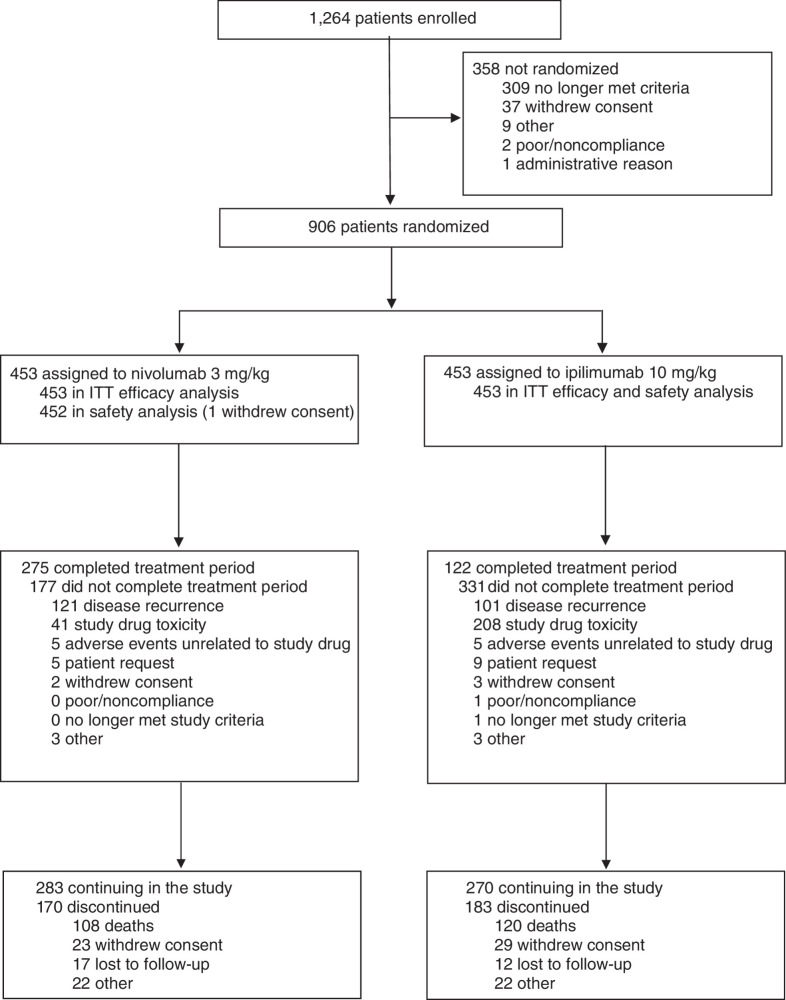
Patients with resected stage IIIB-C/IV melanoma were stratified by stage and baseline programmed death cell ligand 1 (PD-L1) expression and received nivolumab 3 mg/kg every 2 weeks or ipilimumab 10 mg/kg every 3 weeks for four doses and then every 12 weeks, both intravenously for 1 year until disease recurrence, unacceptable toxicity, or withdrawal of consent. The primary endpoint was RFS.
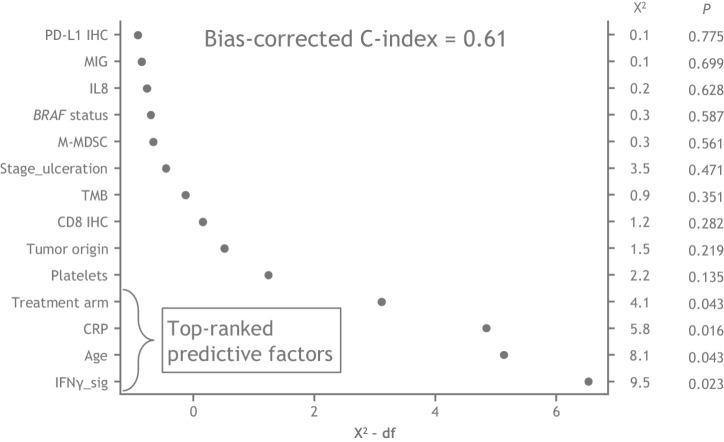
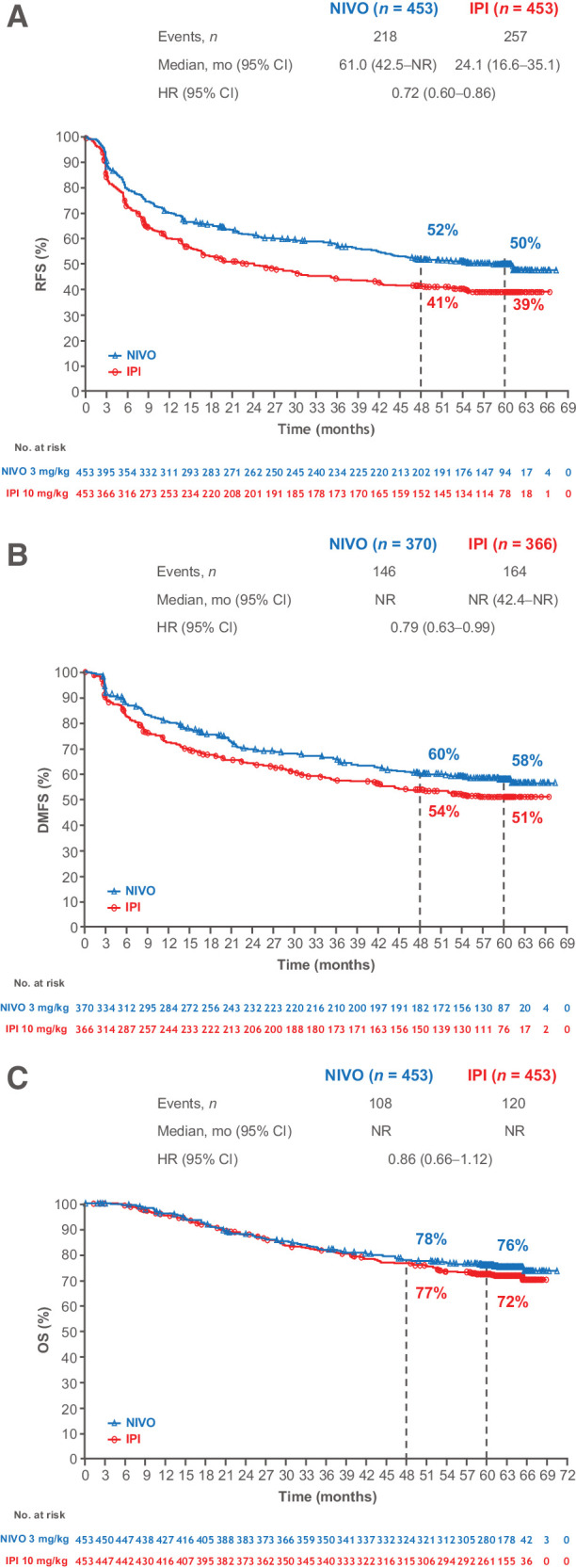
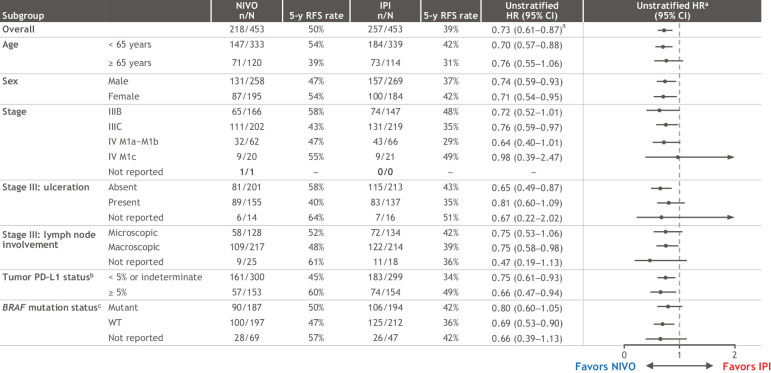
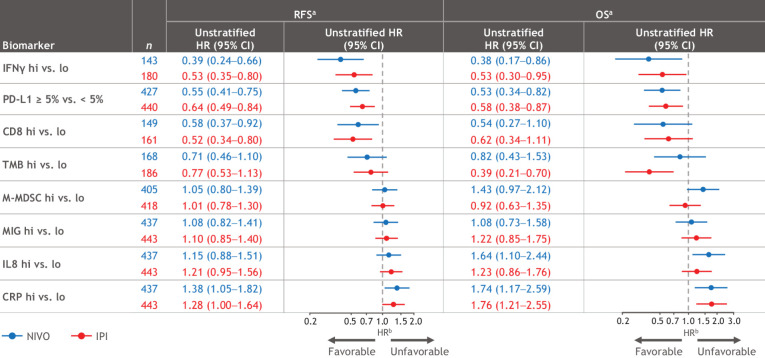
At a minimum follow-up of 62 months, RFS with nivolumab remained superior to ipilimumab (HR = 0.72; 95% confidence interval, 0.60-0.86; 5-year rates of 50% vs. 39%). Five-year distant metastasis-free survival (DMFS) rates were 58% with nivolumab versus 51% with ipilimumab. Five-year overall survival (OS) rates were 76% with nivolumab and 72% with ipilimumab (75% data maturity: 228 of 302 planned events). Higher levels of tumor mutational burden (TMB), tumor PD-L1, intratumoral CD8+ T cells and IFNγ-associated gene expression signature, and lower levels of peripheral serum C-reactive protein were associated with improved RFS and OS with both nivolumab and ipilimumab, albeit with limited clinically meaningful predictive value.
Nivolumab is a proven adjuvant treatment for resected melanoma at high risk of recurrence, with sustained, long-term improvement in RFS and DMFS compared with ipilimumab and high OS rates. Identification of additional biomarkers is needed to better predict treatment outcome. See related commentary by Augustin and Luke, p. 3253.
在 III 期 CheckMate 238 研究中,与伊匹单抗相比,辅助纳武利尤单抗显著改善了 IIIB-C 期或 IV 期黑色素瘤患者的无复发生存 (RFS) 和远处无转移生存 (DMFS),且该获益在 4 年时得以维持。我们报告了更新的 5 年疗效和生物标志物发现。
III 期 IIIB-C/IV 期黑色素瘤患者按分期和基线程序性死亡配体 1(PD-L1)表达进行分层,接受纳武利尤单抗 3mg/kg,每 2 周 1 次,或伊匹单抗 10mg/kg,每 3 周 1 次,共 4 剂,然后每 12 周 1 次,静脉输注 1 年,直至疾病复发、不可接受的毒性或患者撤回同意。主要终点为 RFS。
在至少 62 个月的随访中,纳武利尤单抗的 RFS 仍优于伊匹单抗(HR=0.72;95%置信区间,0.60-0.86;5 年率分别为 50%和 39%)。纳武利尤单抗组的 5 年 DMFS 率为 58%,伊匹单抗组为 51%。纳武利尤单抗组的 5 年总生存(OS)率为 76%,伊匹单抗组为 72%(75%数据成熟度:计划事件 302 例中的 228 例)。较高的肿瘤突变负担(TMB)、肿瘤 PD-L1、肿瘤内 CD8+T 细胞和 IFNγ相关基因表达特征以及较低的外周血 C-反应蛋白水平与纳武利尤单抗和伊匹单抗的 RFS 和 OS 改善相关,尽管具有有限的临床意义预测价值。
纳武利尤单抗是一种已被证实的高复发风险黑色素瘤辅助治疗药物,与伊匹单抗相比,RFS 和 DMFS 持续、长期改善,OS 率高。需要进一步鉴定其他生物标志物,以更好地预测治疗结果。详见 Augustin 和 Luke 的相关述评,第 3253 页。