Department of Biomedical and Clinical Sciences, Division of Inflammation and Infection/Rheumatology, Linköping University, Linköping, Sweden.
Central Hospital in Kristianstad, Department of Infectious Diseases and Department of Clinical Sciences, Section for Rheumatology, Lund University, Lund, Sweden; Department of Clinical Sciences, Lund, Section for Rheumatology, Lund University and Skåne University Hospital, Lund, Sweden.
Vaccine. 2023 May 11;41(20):3247-3257. doi: 10.1016/j.vaccine.2023.03.065. Epub 2023 Apr 4.
To elucidate antibody responses after the second and third dose of COVID-19 vaccine in patients with inflammatory rheumatic diseases (IRD) treated with biologic/targeted disease modifying anti-rheumatic drugs (b/ts DMARDs).
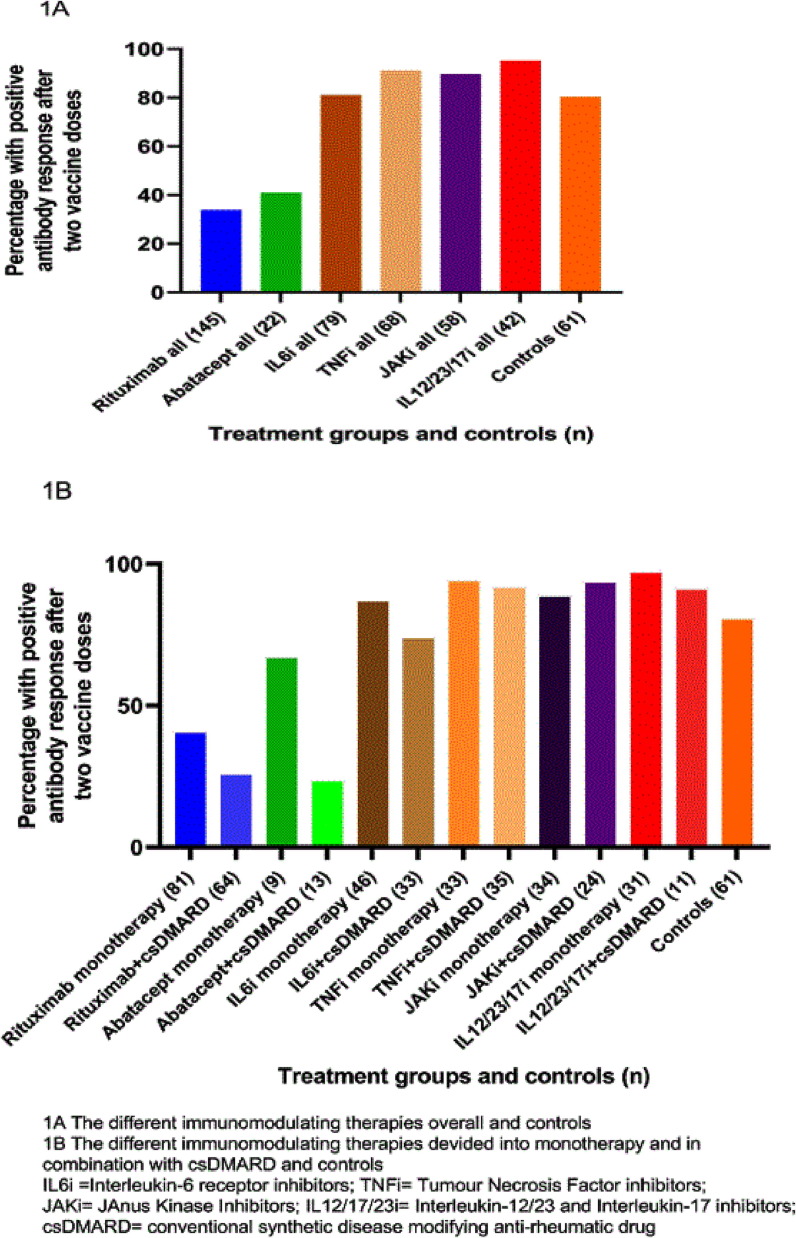
Antibody levels to antigens representing spike full length protein and spike S1 were measured before vaccination, 2-12 weeks after the second dose, before and after the third dose using multiplex bead-based serology assay. Positive antibody response was defined as antibody levels over cut off (seropositivity) in seronegative individuals or ≥ 4-fold increase in antibodies in individuals seropositive for both spike proteins.
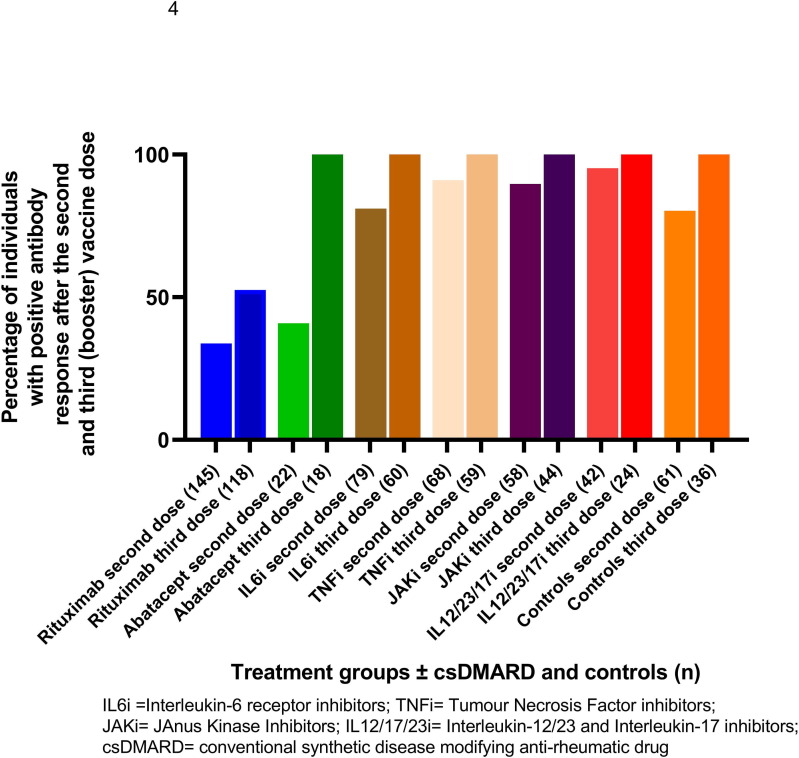
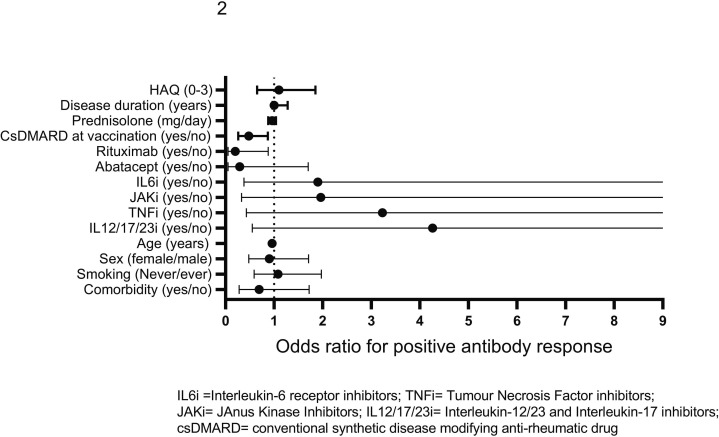
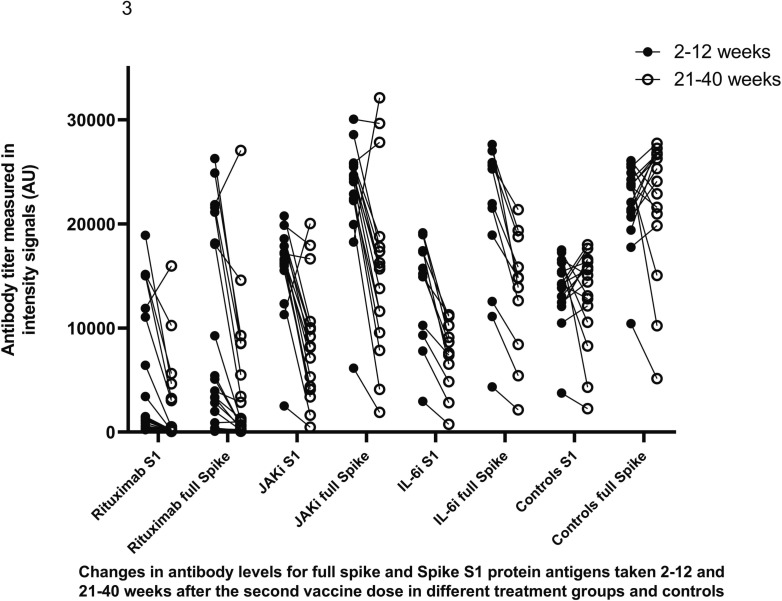
Patients (n = 414) receiving b/ts DMARDs (283 had arthritis, 75 systemic vasculitis and 56 other autoimmune diseases) and controls (n = 61) from five Swedish regions participated. Treatments groups were: rituximab (n = 145); abatacept (n = 22); Interleukin 6 receptor inhibitors [IL6i (n = 79)]; JAnus Kinase Inhibitors [JAKi (n = 58)], Tumour Necrosis Factor inhibitor [TNFi (n = 68)] and Interleukin12/23/17 inhibitors [IL12/23/17i (n = 42)]. Percentage of patients with positive antibody response after two doses was significantly lower in rituximab (33,8%) and abatacept (40,9%) (p < 0,001) but not in IL12/23/17i, TNFi or JAKi groups compared to controls (80,3%). Higher age, rituximab treatment and shorter time between last rituximab course and vaccination predicted impaired antibody response. Antibody levels collected 21-40 weeks after second dose decreased significantly (IL6i: p = 0,02; other groups: p < 0,001) compared to levels at 2-12 week but most participants remained seropositive. Proportion of patients with positive antibody response increased after third dose but was still significantly lower in rituximab (p < 0,001).
Older individuals and patients on maintenance rituximab have an impaired response after two doses of COVID-19 vaccine which improves if the time between last rituximab course and vaccination extends and also after an additional vaccine dose. Rituximab patients should be prioritized for booster vaccine doses. TNFi, JAKi and IL12/23/17i does not diminished humoral response to primary and an additional vaccination.
阐明在接受生物/靶向疾病修正抗风湿药物(b/ts DMARDs)治疗的炎症性风湿病(IRD)患者中,COVID-19 疫苗第二和第三剂后的抗体反应。
使用基于多重珠的血清学检测法,在接种疫苗前、第二剂后 2-12 周、第三剂前和第三剂后测量代表刺突全长蛋白和刺突 S1 的抗原的抗体水平。将抗体水平超过截止值(血清阳性)的血清阴性个体或两种刺突蛋白均为血清阳性的个体的抗体水平增加≥4 倍定义为阳性抗体反应。
来自瑞典五个地区的 414 名接受 b/ts DMARDs 治疗的患者(283 名患有关节炎,75 名患有系统性血管炎,56 名患有其他自身免疫性疾病)和 61 名对照者参加了这项研究。治疗组包括:利妥昔单抗(n=145);阿巴西普(n=22);白细胞介素 6 受体抑制剂[IL6i(n=79)];Janus 激酶抑制剂[JAKi(n=58)];肿瘤坏死因子抑制剂[TNiFi(n=68)]和白细胞介素 12/23/17 抑制剂[IL12/23/17i(n=42)]。与对照组相比,两剂后血清阳性抗体反应的患者比例显著降低,利妥昔单抗(33.8%)和阿巴西普(40.9%)(p<0.001),但 IL12/23/17i、TNiFi 或 JAKi 组并非如此(80.3%)。较高的年龄、利妥昔单抗治疗和最后一次利妥昔单抗疗程与接种疫苗之间的时间较短预测抗体反应受损。与 2-12 周时的水平相比,第二次剂量后 21-40 周采集的抗体水平显著下降(IL6i:p=0.02;其他组:p<0.001),但大多数参与者仍为血清阳性。第三剂后血清阳性抗体反应的比例增加,但利妥昔单抗仍显著降低(p<0.001)。
年龄较大的个体和接受维持性利妥昔单抗治疗的患者在接受 COVID-19 疫苗两剂后反应受损,如果最后一次利妥昔单抗疗程与接种疫苗之间的时间延长,并且接受额外的疫苗剂量,反应会有所改善。利妥昔单抗患者应优先接种加强疫苗。TNFi、JAKi 和 IL12/23/17i 不会降低对初次和额外接种的体液反应。