Wang Mawson, Seibel Markus J
Department of Endocrinology and Metabolism, Concord Hospital, Sydney, Australia.
Concord Clinical School, Faculty of Medicine and Health, University of Sydney, Sydney, Australia.
Endocrinol Diabetes Metab Case Rep. 2023 May 11;2023(2). doi: 10.1530/EDM-22-0408. Print 2023 May 1.
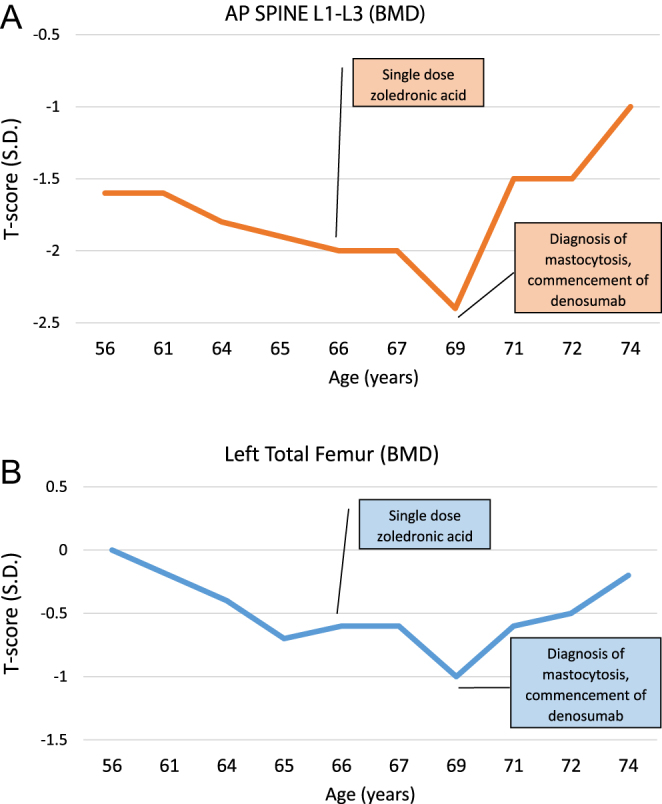
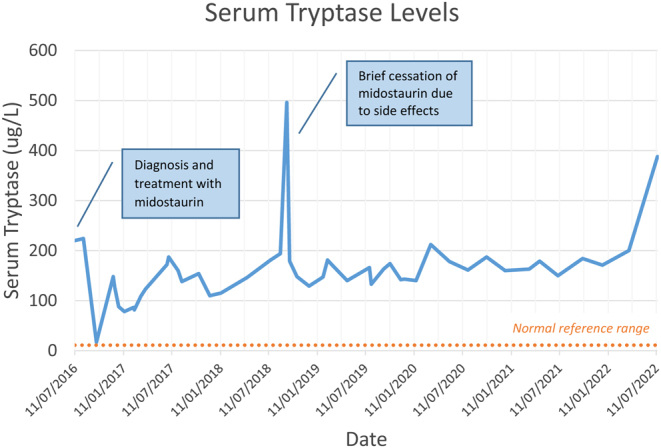
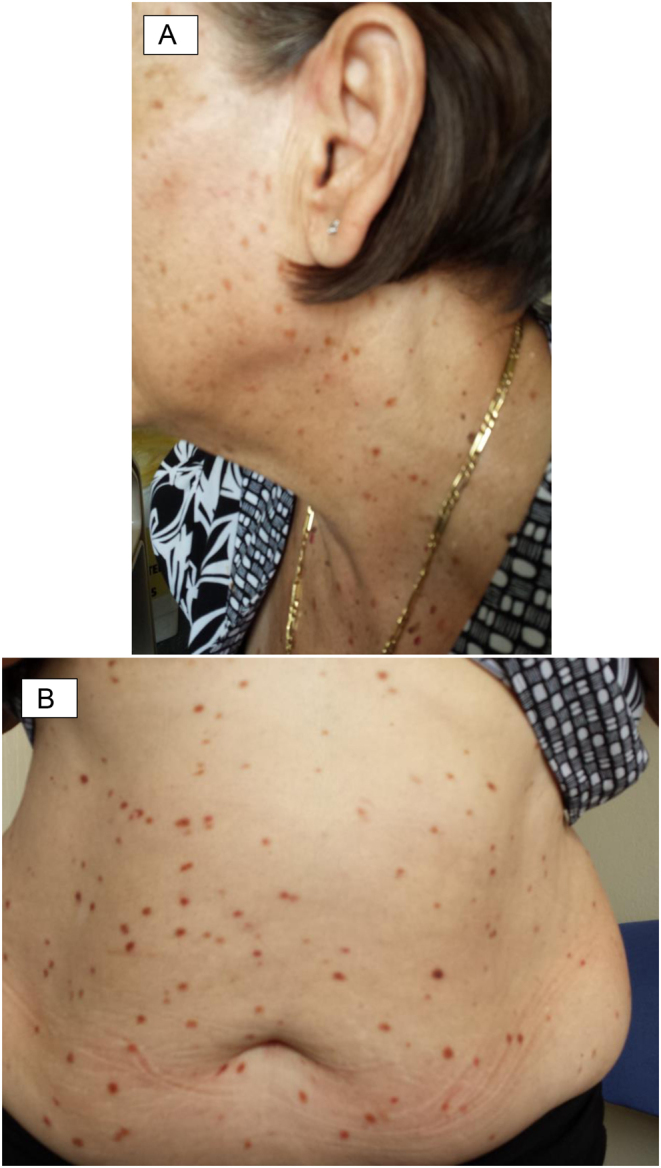
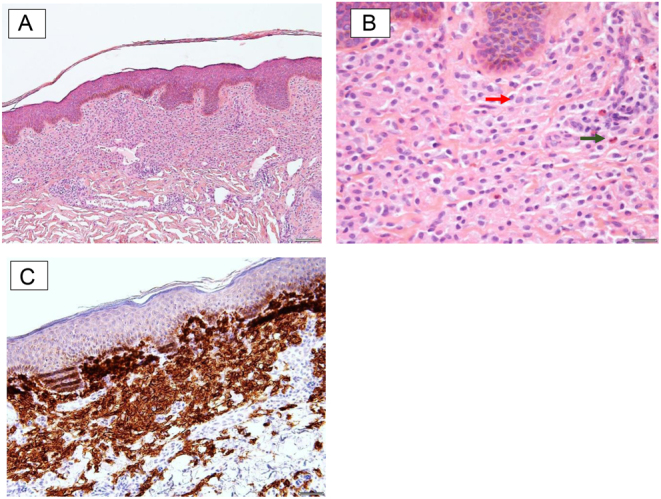
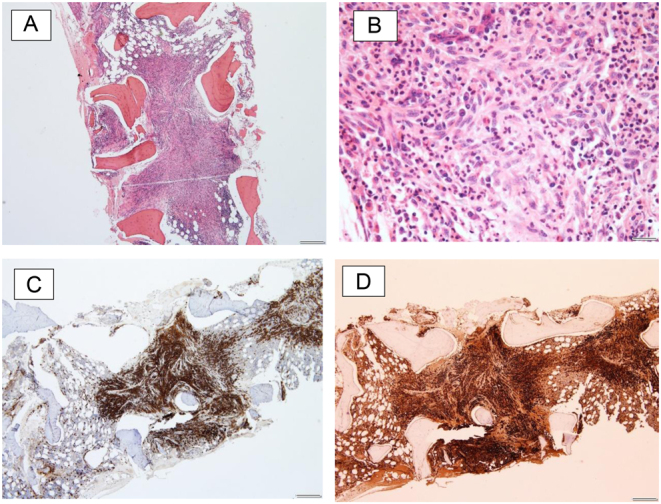
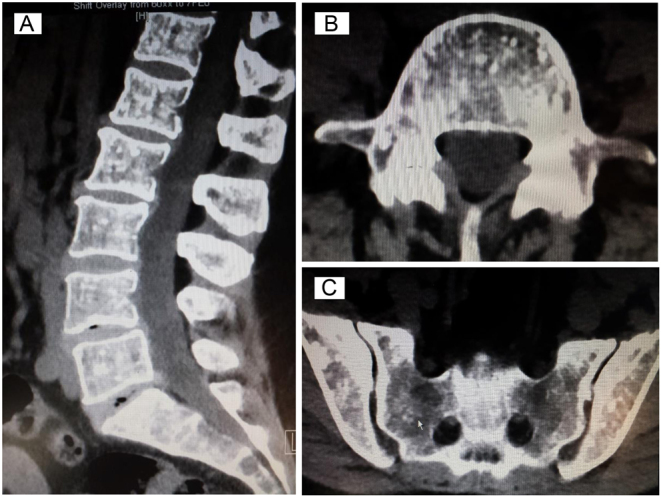
We report the case of a 69-year-old female with systemic mastocytosis, diagnosed based on widespread pigmented papules and macules, elevated serum tryptase levels and confirmatory skin and bone marrow biopsy, on a background of osteoporosis. A CT demonstrated multiple sclerotic lesions within lumbar vertebral bodies, sacrum and ileum, with surrounding osteolysis but no obvious compression fractures. She was treated with the RANK-L inhibitor denosumab, resulting in significant bone mineral density gain over the following 5 years. However, her serum tryptase levels gradually increased during this period despite treatment with the multikinase inhibitor, midostaurin. It is thus conceivable that her rapid increase in bone mineral density may be partly contributed by a predominance of pro-osteoblastic mediators released by abnormal mast cells, suggestive of more advanced disease. This case highlights the complexities of systemic mastocytosis-related bone disease and the interplay of numerous mediators contributing to a phenotype of both increased bone resorption and formation.
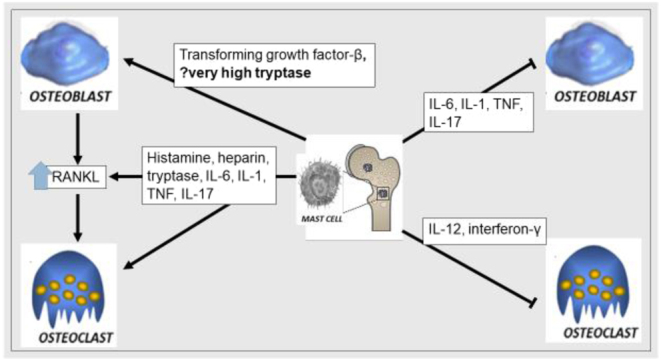
Systemic mastocytosis is a neoplastic disease of mast cells characterized by abnormal proliferation and accumulation in the skin and other organs. It is most frequently associated with the somatic gain-of-function KIT D816V mutation. Systemic mastocytosis should be suspected in patients presenting with not only cutaneous symptoms suggestive of mast cell degranulation such as anaphylaxis, flushing or urticaria but also unexplained osteoporosis and gastrointestinal and constitutional symptoms. The prevalence of osteoporosis in systemic mastocytosis is high. Mast cell activation leads to the secretion of numerous chemical mediators which either promote or inhibit osteoclastic and/or osteoblastic activity, with the balance usually in favour of increased bone resorption. However, in advanced diseases with high mast cell burden, mast-cell-derived cytokines and mediators may promote osteoblastic activity, leading to osteosclerosis and apparent increases in bone mineral density. Treatment of osteoporosis in systemic mastocytosis involves antiresorptive therapy with bisphosphonates and more recently, denosumab. There are limited data on the role of osteoanabolic agents.
我们报告了一例69岁患有系统性肥大细胞增多症的女性病例。该病例基于广泛分布的色素沉着丘疹和斑疹、血清类胰蛋白酶水平升高以及确诊性的皮肤和骨髓活检确诊,其背景为骨质疏松症。CT显示腰椎椎体、骶骨和回肠内有多个硬化性病变,周围有骨质溶解,但无明显压缩性骨折。她接受了RANK-L抑制剂地诺单抗治疗,在接下来的5年里骨矿物质密度显著增加。然而,尽管使用了多激酶抑制剂米哚妥林进行治疗,在此期间她的血清类胰蛋白酶水平仍逐渐升高。因此可以推测,她骨矿物质密度的快速增加可能部分归因于异常肥大细胞释放的促骨形成介质占主导,这提示疾病更为进展。该病例突出了系统性肥大细胞增多症相关骨病的复杂性以及众多介质之间的相互作用,这些介质共同导致了骨吸收和形成增加的表型。
系统性肥大细胞增多症是一种肥大细胞的肿瘤性疾病,其特征是在皮肤和其他器官中异常增殖和积聚。它最常与体细胞功能获得性KIT D816V突变相关。对于不仅出现提示肥大细胞脱颗粒的皮肤症状(如过敏反应、潮红或荨麻疹),还伴有不明原因的骨质疏松以及胃肠道和全身症状的患者,应怀疑患有系统性肥大细胞增多症。系统性肥大细胞增多症中骨质疏松症的患病率很高。肥大细胞活化导致多种化学介质的分泌,这些介质要么促进要么抑制破骨细胞和/或成骨细胞的活性,通常平衡偏向于骨吸收增加。然而,在肥大细胞负荷高的晚期疾病中,肥大细胞衍生的细胞因子和介质可能促进成骨细胞活性,导致骨质硬化和骨矿物质密度明显增加。系统性肥大细胞增多症中骨质疏松症的治疗包括使用双膦酸盐进行抗吸收治疗,以及最近使用的地诺单抗。关于骨合成代谢药物作用的数据有限。