Mie Takafumi, Sasaki Takashi, Okamoto Takeshi, Takeda Tsuyoshi, Mori Chinatsu, Yamada Yuto, Furukawa Takaaki, Kasuga Akiyoshi, Matsuyama Masato, Ozaka Masato, Sasahira Naoki
Department of Hepato-Biliary-Pancreatic Medicine, Cancer Institute Hospital of Japanese Foundation for Cancer Research, Tokyo, Japan.
Clin Endosc. 2024 Mar;57(2):253-262. doi: 10.5946/ce.2022.216. Epub 2023 May 16.
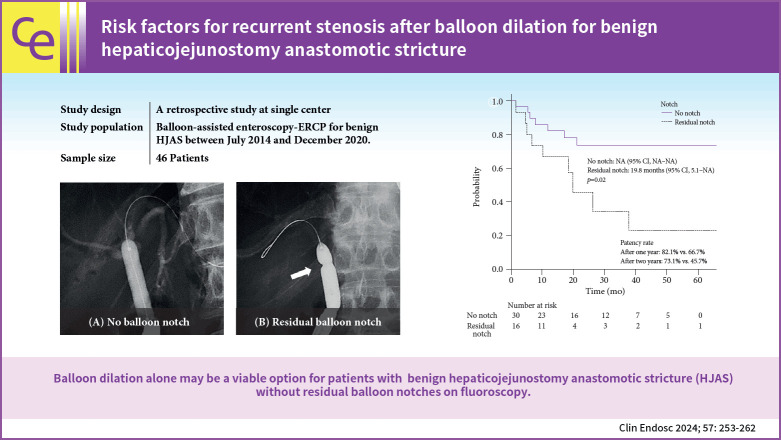
BACKGROUND/AIMS: Hepaticojejunostomy anastomotic stricture (HJAS) is a feared adverse event associated with hepatopancreatobiliary surgery. Although balloon dilation for benign HJAS during endoscopic retrograde cholangiopancreatography with balloon-assisted enteroscopy has been reported to be useful, the treatment strategy remains controversial. Therefore, we evaluated the outcomes and risk factors of recurrent stenosis after balloon dilation alone for benign HJAS.
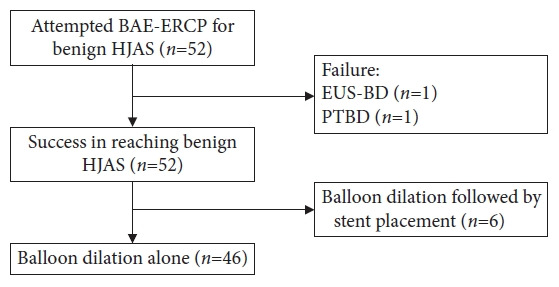
We retrospectively analyzed consecutive patients who underwent balloon-assisted enteroscopy-endoscopic retrograde cholangiopancreatography for benign HJAS at our institution between July 2014 and December 2020.
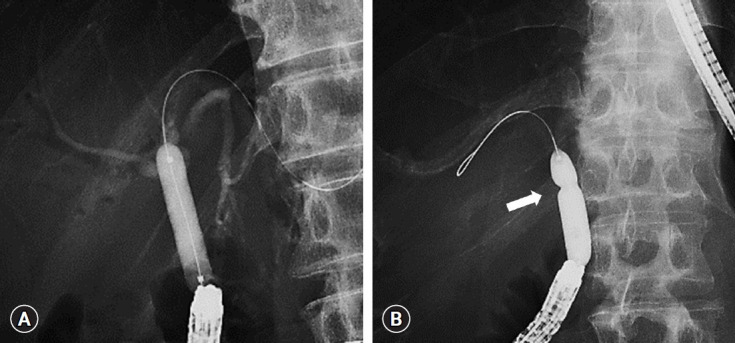
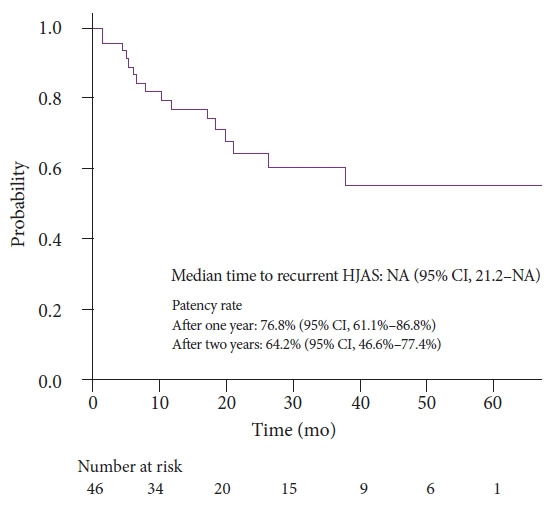
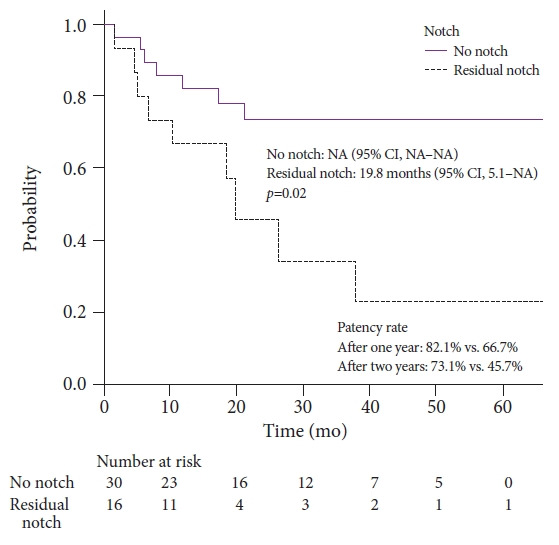
Forty-six patients were included, 16 of whom had recurrent HJAS after balloon dilation. The patency rates at 1 and 2 years after balloon dilation were 76.8% and 64.2%, respectively. Presence of a residual balloon notch during balloon dilation was an independent predictor of recurrence (hazard ratio, 2.80; 95% confidence interval, 1.01-7.78; p=0.048), whereas HJAS within postoperative 1 year tended to be associated with recurrence (hazard ratio, 2.43; 95% confidence interval, 0.85-6.89; p=0.096). The patency rates in patients without a residual balloon notch were 82.1% and 73.1% after 1 and 2 years, respectively.
Balloon dilation alone may be a viable option for patients with benign HJAS without residual balloon notches on fluoroscopy.
背景/目的:肝空肠吻合口狭窄(HJAS)是肝胆胰外科手术中令人担忧的不良事件。尽管有报道称在内镜逆行胰胆管造影术联合球囊辅助小肠镜检查期间对良性HJAS进行球囊扩张是有效的,但治疗策略仍存在争议。因此,我们评估了单纯球囊扩张治疗良性HJAS后再狭窄的结局和危险因素。
我们回顾性分析了2014年7月至2020年12月在我院因良性HJAS接受球囊辅助小肠镜检查-内镜逆行胰胆管造影术的连续患者。
纳入46例患者,其中16例在球囊扩张后出现复发性HJAS。球囊扩张后1年和2年的通畅率分别为76.8%和64.2%。球囊扩张期间存在残留球囊切迹是复发的独立预测因素(风险比,2.80;95%置信区间,1.01-7.78;p=0.048),而术后1年内出现的HJAS往往与复发相关(风险比,2.43;95%置信区间,0.85-6.89;p=0.096)。无残留球囊切迹患者的1年和2年通畅率分别为82.1%和73.1%。
对于在荧光透视下无残留球囊切迹的良性HJAS患者,单纯球囊扩张可能是一种可行的选择。