Division of Neonatology, The Children's Hospital of Philadelphia, Philadelphia, Pennsylvania.
Leonard Davis Institute of Health Economics, Philadelphia, Pennsylvania.
JAMA Netw Open. 2023 May 1;6(5):e2315306. doi: 10.1001/jamanetworkopen.2023.15306.
Appreciation for the effects of neighborhood conditions and community factors on perinatal health is increasing. However, community-level indices specific to maternal health and associations with preterm birth (PTB) have not been assessed.
To examine the association of the Maternal Vulnerability Index (MVI), a novel county-level index designed to quantify maternal vulnerability to adverse health outcomes, with PTB.
DESIGN, SETTING, AND PARTICIPANTS: This retrospective cohort study used US Vital Statistics data from January 1 to December 31, 2018. Participants included 3 659 099 singleton births at 22 plus 0/7 to 44 plus 6/7 weeks of gestation born in the US. Analyses were conducted from December 1, 2021, through March 31, 2023.
The MVI, a composite measure of 43 area-level indicators, categorized into 6 themes reflecting physical, social, and health care landscapes. Overall MVI and theme were stratified by quintile (very low to very high) by maternal county of residence.
The primary outcome was PTB (gestational age <37 weeks). Secondary outcomes were PTB categories: extreme (gestational age ≤28 weeks), very (gestational age 29-31 weeks), moderate (gestational age 32-33 weeks), and late (gestational age 34-36 weeks). Multivariable logistic regression quantified associations of MVI, overall and by theme, with PTB, overall and by PTB category.
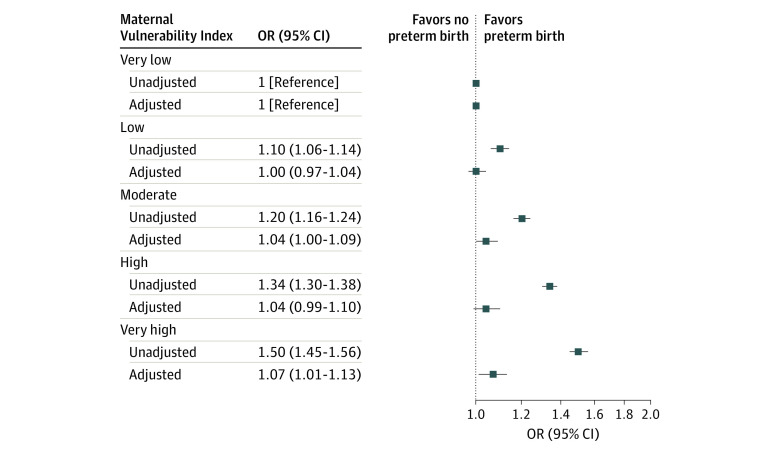
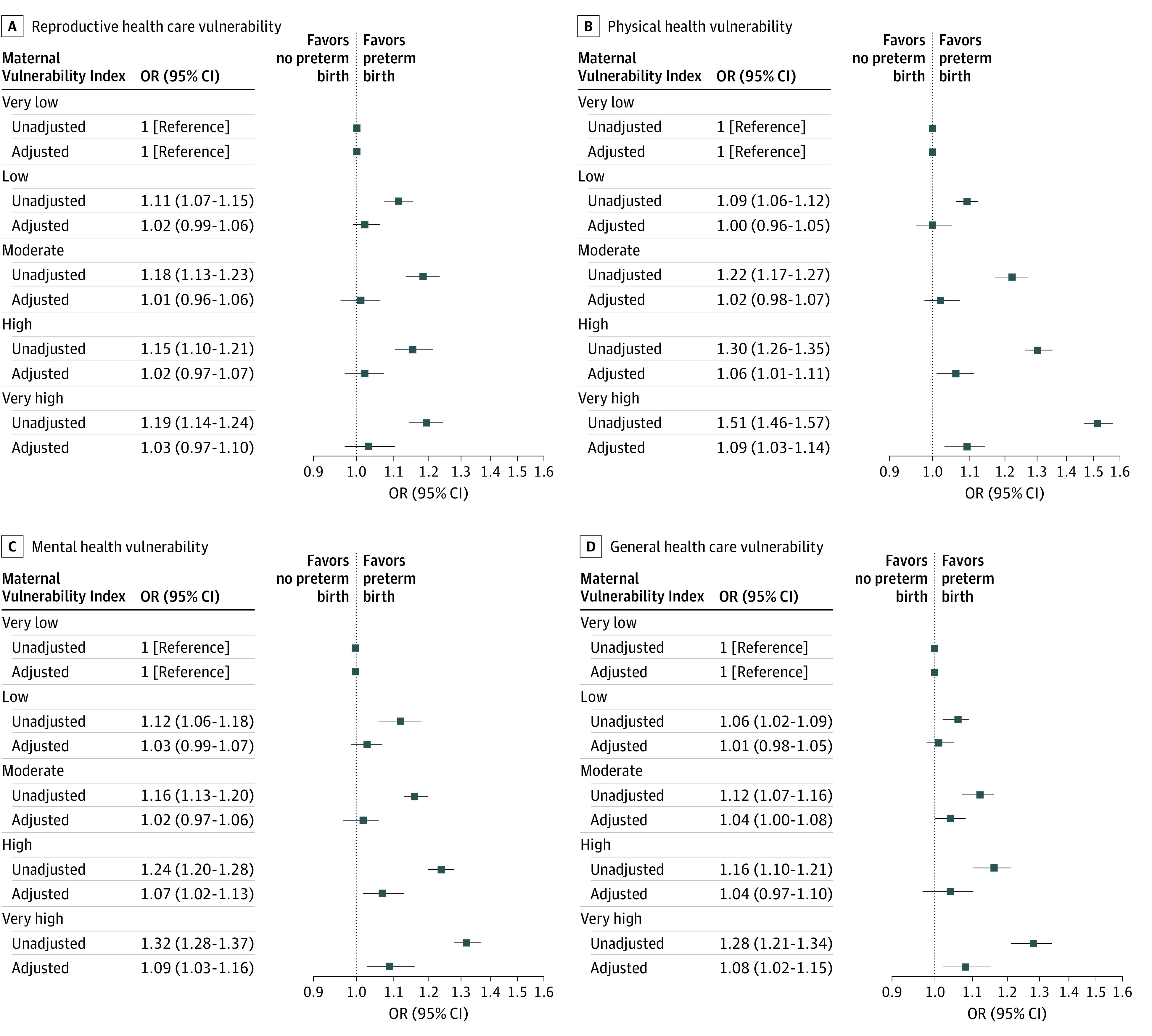
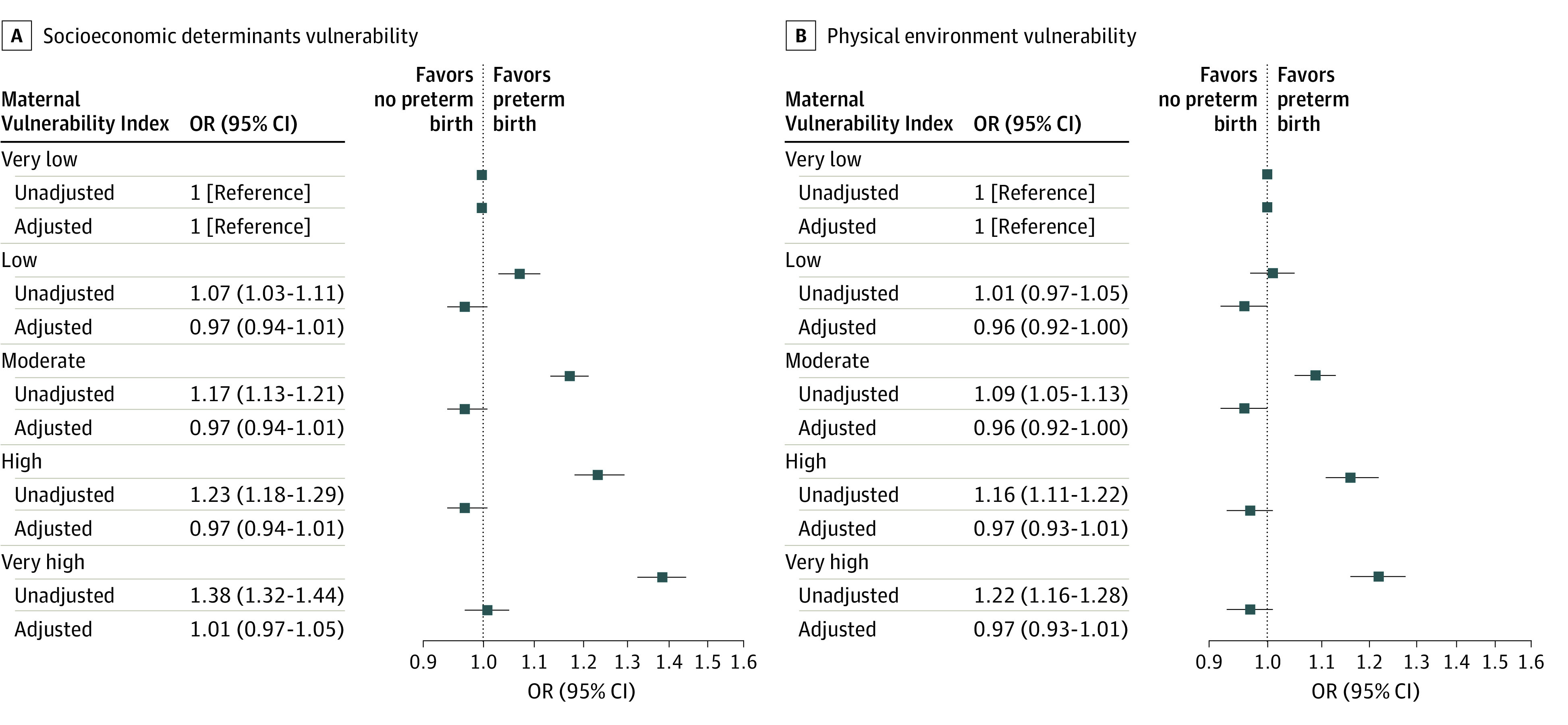
Among 3 659 099 births, 298 847 (8.2%) were preterm (male, 51.1%; female, 48.9%). Maternal race and ethnicity included 0.8% American Indian or Alaska Native, 6.8% Asian or Pacific Islander, 23.6% Hispanic, 14.5% non-Hispanic Black, 52.1% non-Hispanic White, and 2.2% with more than 1 race. Compared with full-term births, MVI was higher for PTBs across all themes. Very high MVI was associated with increased PTB in unadjusted (odds ratio [OR], 1.50 [95% CI, 1.45-1.56]) and adjusted (OR, 1.07 [95% CI, 1.01-1.13]) analyses. In adjusted analyses of PTB categories, MVI had the largest association with extreme PTB (adjusted OR, 1.18 [95% CI, 1.07-1.29]). Higher MVI in the themes of physical health, mental health and substance abuse, and general health care remained associated with PTB overall in adjusted models. While the physical health and socioeconomic determinant themes were associated with extreme PTB, physical health, mental health and substance abuse, and general health care themes were associated with late PTB.
The findings of this cohort study suggest that MVI was associated with PTB even after adjustment for individual-level confounders. The MVI is a useful measure for county-level PTB risk that may have policy implications for counties working to lower preterm rates and improve perinatal outcomes.
人们越来越意识到社区条件和社区因素对围产期健康的影响。然而,专门针对孕产妇健康的社区层面指数及其与早产(PTB)的关联尚未得到评估。
本研究旨在评估孕产妇脆弱性指数(MVI)与 PTB 的关系,MVI 是一种新的县级指数,旨在量化孕产妇对不良健康结果的脆弱性。
设计、地点和参与者:本回顾性队列研究使用了美国 2018 年 1 月 1 日至 12 月 31 日期间的美国人口普查局数据。参与者包括 3659099 名在妊娠 22 加 0/7 至 44 加 6/7 周时单胎分娩的母亲,这些母亲均在美国出生。分析于 2021 年 12 月 1 日至 2023 年 3 月 31 日进行。
MVI 是 43 个区域水平指标的综合衡量指标,分为 6 个主题,反映了物理、社会和医疗保健环境。根据母亲居住的县,对整体 MVI 和主题进行五分位数(非常低至非常高)分层。
主要结局是 PTB(胎龄<37 周)。次要结局是 PTB 类别:极早产(胎龄≤28 周)、非常早产(胎龄 29-31 周)、中度早产(胎龄 32-33 周)和晚期早产(胎龄 34-36 周)。多变量逻辑回归量化了 MVI 与 PTB 的关联,整体和按 PTB 类别进行分析。
在 3659099 例分娩中,298847 例(8.2%)为早产(男性,51.1%;女性,48.9%)。母亲的种族和民族包括 0.8%的美洲印第安人或阿拉斯加原住民、6.8%的亚洲或太平洋岛民、23.6%的西班牙裔、14.5%的非西班牙裔黑人、52.1%的非西班牙裔白人,以及 2.2%的多种族。与足月分娩相比,MVI 在所有主题中均与 PTB 呈正相关。未经调整(比值比[OR],1.50[95%置信区间,1.45-1.56])和调整(OR,1.07[95%置信区间,1.01-1.13])分析中,高 MVI 与 PTB 相关。在调整后的 PTB 类别分析中,MVI 与极早产的关联最大(调整后的 OR,1.18[95%置信区间,1.07-1.29])。在调整后的模型中,健康和社会经济决定因素主题与整体 PTB 相关,而物理健康、心理健康和物质滥用以及一般医疗保健主题与晚期 PTB 相关。
这项队列研究的结果表明,即使在调整了个体水平的混杂因素后,MVI 与 PTB 仍相关。MVI 是衡量县级 PTB 风险的有用指标,这可能对致力于降低早产率和改善围产期结局的县具有政策意义。