Yap Desmond Y H, Lie Davina, Lau Tiffany, Tang Alex, Chan Gavin, Chan Thomas S Y, Sim Joycelyn, Lie Albert K W, Chan Tak Mao
Division of Nephrology, Department of Medicine, Queen Mary Hospital, The University of Hong Kong, Hong Kong.
Department of Pathology, Queen Mary Hospital, The University of Hong Kong, Hong Kong.
Clin Kidney J. 2022 Dec 10;16(6):976-984. doi: 10.1093/ckj/sfac264. eCollection 2023 Jun.
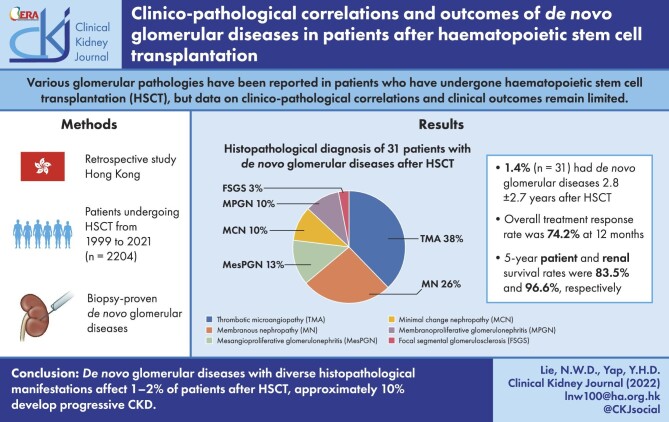
Various glomerular pathologies have been reported in patients who have undergone haematopoietic stem cell transplantation (HSCT), but the data on clinico-pathological correlations and clinical outcome remain limited.
We analysed the clinical and histopathological data of patients who had biopsy-proven glomerular diseases after HSCT since 1999.
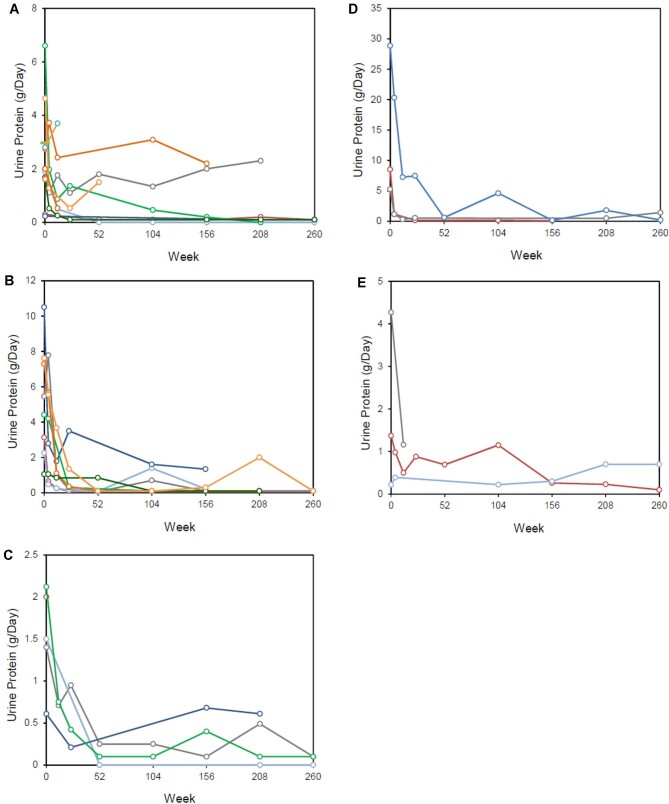
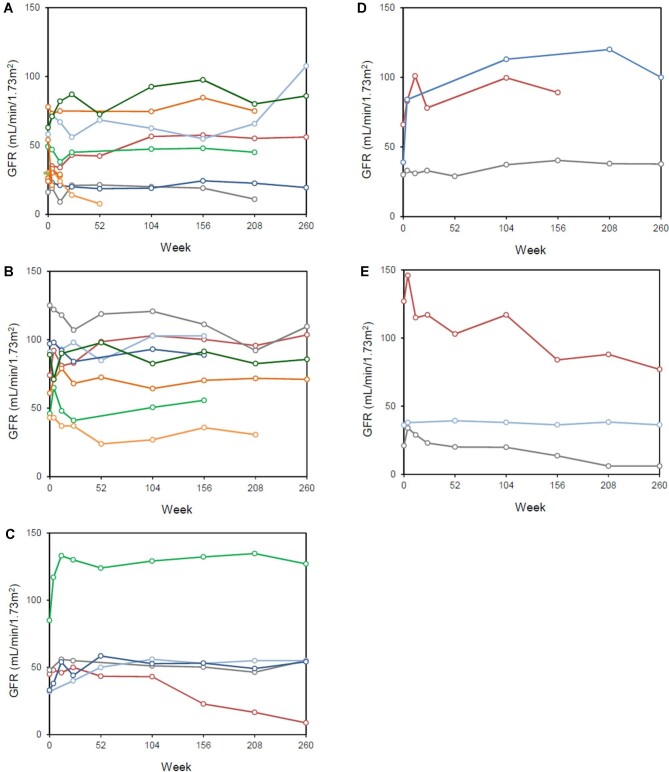
A total of 2204 patients underwent HSCT during the period 1999-2021, and 31 patients (1.4%) developed glomerular diseases after a mean duration of 2.8 ± 2.7 years after HSCT. Fifteen of these patients (48.4%) had graft-versus-host-disease prior to or concomitant with renal abnormalities. Proteinuria and eGFR at the time of kidney biopsy were 4.1 ± 5.3 g/day and 50.8 ± 25.4 mL/min/1.73 m, respectively. Kidney histopathologic diagnoses included thrombotic microangiopathy (TMA) (38.7%), membranous nephropathy (MN) (25.8%), mesangial proliferative glomerulonephritis (12.9%), minimal change disease (9.7%), focal segmental glomerulosclerosis (9.7%) and membranoproliferative glomerulonephritis (3.2%). Immunosuppressive treatment was given to patients who presented with nephrotic-range proteinuria and/or acute kidney injury, while renin-angiotensin-aldosterone blockade was given to all patients with proteinuria ≥1 g/day, with complete and partial response rates of 54.8% and 19.4%, respectively. One patient with TMA progressed to end-stage kidney disease after 24 weeks, and two patients, one with TMA and one with MN, (6.4%) progressed to chronic kidney disease (CKD) Stage ≥3. Kidney and patient survival rates were 96.6% and 83.5%, respectively, at 5 years.
glomerular diseases with diverse histopathologic manifestations affect 1.4% of patients after HSCT, and approximately 10% develop progressive CKD.
造血干细胞移植(HSCT)患者中已报告了多种肾小球病变,但临床病理相关性和临床结局的数据仍然有限。
我们分析了自1999年以来经活检证实患有HSCT后肾小球疾病患者的临床和组织病理学数据。
1999年至2021年期间共有2204例患者接受了HSCT,31例患者(1.4%)在HSCT后平均2.8±2.7年出现肾小球疾病。其中15例患者(48.4%)在肾脏异常之前或同时患有移植物抗宿主病。肾活检时的蛋白尿和估算肾小球滤过率(eGFR)分别为4.1±5.3g/天和50.8±25.4mL/min/1.73m²。肾脏组织病理学诊断包括血栓性微血管病(TMA)(38.7%)、膜性肾病(MN)(25.8%)、系膜增生性肾小球肾炎(12.9%)、微小病变病(9.7%)、局灶节段性肾小球硬化(9.7%)和膜增生性肾小球肾炎(3.2%)。对出现肾病范围蛋白尿和/或急性肾损伤的患者给予免疫抑制治疗;对所有蛋白尿≥1g/天的患者给予肾素-血管紧张素-醛固酮阻滞剂治疗,完全缓解率和部分缓解率分别为54.8%和19.4%。1例TMA患者在24周后进展为终末期肾病,2例患者(1例TMA和1例MN)(6.4%)进展为慢性肾脏病(CKD)3期及以上。5年时肾脏和患者生存率分别为96.6%和83.5%。
具有多种组织病理学表现的肾小球疾病影响1.4%的HSCT后患者,约10%发展为进行性CKD。