Department of Orthopaedics and Traumatology, University Hospital Basel, Spitalstrasse 21, 4031, Basel, Switzerland.
Department of Clinical Research, University of Basel, Schanzenstrasse 55, 4056, Basel, Switzerland.
Arch Orthop Trauma Surg. 2023 Oct;143(10):6147-6157. doi: 10.1007/s00402-023-04923-w. Epub 2023 Jun 6.
The aim of this study was to describe the indications and technical aspects of medial closing and lateral opening distal femoral osteotomy (MCDFO and LODFO) for patients with a valgus knee and to report clinical and radiological outcomes and complications.
Over 6 years, 28 DFOs (22 MCDFO, 6 LODFO) were performed in 22 Patients. In this cohort study, we retrospectively analyzed clinical and radiological outcome measures as well as complications.
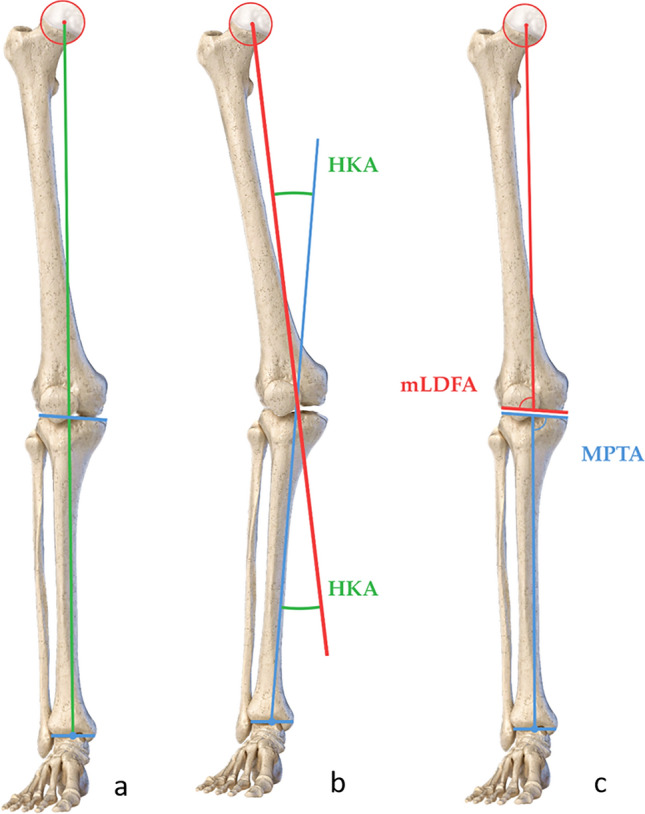
The median (range) age was 47 (17-63) years, height 1.68 (1.56-1.98) m, body mass 80 (49-105) kg, and body mass index (BMI) 27.4 (18.6-37.0) kg/m. The clinical follow-up was 21 (7-81) months, the need for total or unicompartmental knee arthroplasty (TKA/UKA) and hardware removal was followed up for 59 (7-108) months postoperatively. Preoperatively, hip-knee-ankle angle (HKA, negative values denote varus) was 7.0 (2.0-13.0)°, mechanical lateral distal femoral angle (mLDFA) was 83.7 (79.9-88.2)°, and mechanical proximal tibial angle (MPTA) was 89.0 (86.6-94.5)°. Postoperatively, HKA was -1.3 (-9.0-1.2)° and mLDFA was 90.8 (87.3-97.3)°. The incidence of minor and major complications was 25% and 14%, the incidence of delayed and nonunion was 18% and 4%, respectively. At the last follow-up, 18% of the patients had pain at rest, 25% during activities of daily living, and 39% during physical activity, and 71% were satisfied with the outcome. 7% of the cases received a TKA/UKA, 71% received a hardware removal.
DFO is a reasonable treatment for lateral osteoarthritis in younger patients to avoid disease progression and the need for an UKA/TKA. However, there is a long rehabilitation time, a considerable risk for complications, and a high need for hardware removal. While many patients experienced symptoms at the long-term follow-up, most were satisfied with the outcome. Appropriate patient information is essential. Level of evidence Level IV, Case Series. Trial registration number NCT04382118, clinicaltrials.gov, May 11, 2020.
本研究旨在描述用于治疗膝外翻患者的股骨远端内侧闭合外侧撑开截骨术(MCDFO 和 LODFO)的适应证和技术要点,并报告临床和影像学结果及并发症。
在超过 6 年的时间里,对 22 名患者的 28 例 DFO(22 例 MCDFO,6 例 LODFO)进行了手术。在这项回顾性队列研究中,我们分析了临床和影像学结果以及并发症。
中位(范围)年龄为 47(17-63)岁,身高 1.68(1.56-1.98)m,体重 80(49-105)kg,体重指数(BMI)27.4(18.6-37.0)kg/m。临床随访时间为 21(7-81)个月,全膝关节置换术(TKA)/单髁膝关节置换术(UKA)和内固定取出的需要时间为术后 59(7-108)个月。术前髋膝踝角(HKA,负值表示外翻)为 7.0(2.0-13.0)°,机械外侧股骨远端角(mLDFA)为 83.7(79.9-88.2)°,机械胫骨近端角(MPTA)为 89.0(86.6-94.5)°。术后 HKA 为-1.3(-9.0-1.2)°,mLDFA 为 90.8(87.3-97.3)°。轻微和严重并发症的发生率分别为 25%和 14%,延迟愈合和不愈合的发生率分别为 18%和 4%。末次随访时,18%的患者有静息痛,25%的患者在日常生活中有疼痛,39%的患者在体力活动中有疼痛,71%的患者对结果满意。7%的患者接受了 TKA/UKA,71%的患者接受了内固定取出。
DFO 是治疗年轻患者外侧骨关节炎的一种合理方法,可以避免疾病进展和需要 UKA/TKA。然而,康复时间长,并发症风险大,内固定取出率高。尽管许多患者在长期随访中出现症状,但大多数患者对结果满意。适当的患者信息是必要的。证据水平 IV,病例系列。试验注册号 NCT04382118,clinicaltrials.gov,2020 年 5 月 11 日。