Department of Pediatrics, Severance Children's Hospital, Yonsei University College of Medicine, Seoul, South Korea; Institute for Immunology and Immunological Diseases, Yonsei University College of Medicine, Seoul, South Korea.
Artificial Intelligence and Big Data Convergence Center, Gil Medical Center, Gachon University College of Medicine, Incheon, South Korea.
Int J Infect Dis. 2023 Sep;134:220-227. doi: 10.1016/j.ijid.2023.06.016. Epub 2023 Jun 21.
The risk of severe COVID-19 in children with a solid organ transplant (SOT) is not well established. We compare the relative risk of severe COVID-19 infection between pediatric SOT and non-SOT children.
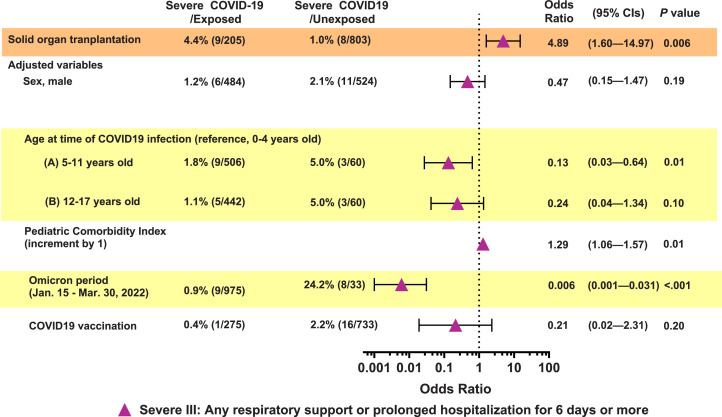
The newly constructed K-COV-N cohort (Korea Disease Control and Prevention Agency-COVID-19-National Health Insurance Service) was used. Children with COVID-19 (<18 years old) who underwent SOT between January 2008 to January 2022 were included. Non-SOT children with COVID-19 were selected in a ratio of 1:4 using propensity score matching. Three definitions of severe COVID-19 were established based on their requirement for respiratory support: severe I (requiring respiratory support above a high-flow nasal cannula or prolonged hospitalization ≥6 days), severe II (requiring any oxygen supplement), and severe III (requiring any oxygen supplement or prolonged hospitalization ≥6 days).
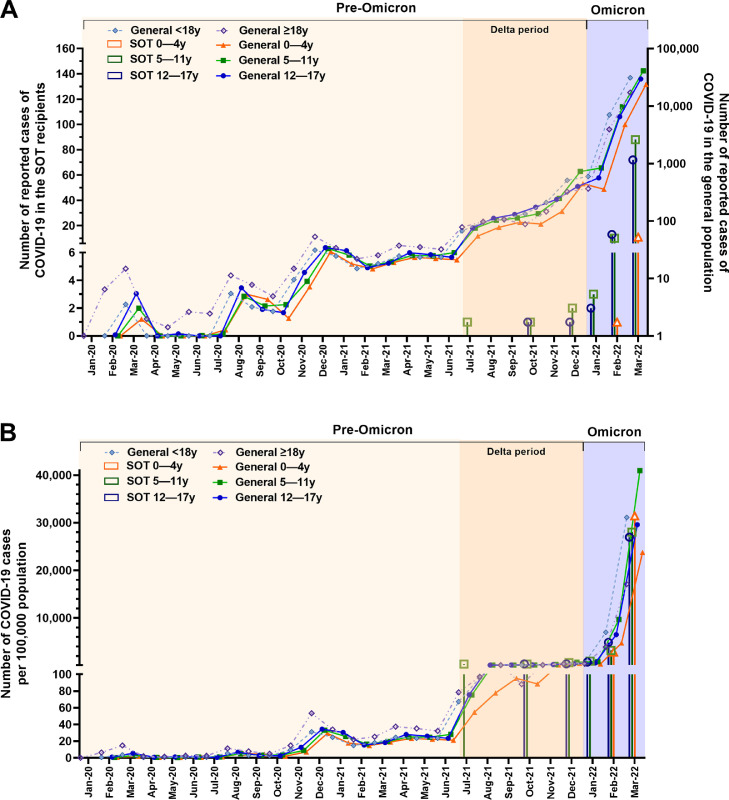
Among 2,957,323 children with COVID-19, 206 pediatric SOT recipients (SOTRs) were identified and included in the analysis along with 803 matched non-SOT children. Most infections (96.6%) occurred during the Omicron period; no cases of mortality were reported. Pediatric SOTR had a 3.6-fold (95% confidence interval = 1.1-11.7, P = 0.03) higher risk of severe I, and a 4.9-fold (95% confidence interval = 1.6-15.0, P = 0.006) higher risk of severe III than non-SOT children. No cases of severe II occurred in the non-SOT children. Although not statistically significant, no severe COVID-19 cases were reported in the vaccinated SOT group (0.0% vs 5.7%, P = 0.09 in severe III).
Pediatric SOTRs have a significantly higher risk of severe COVID-19 than non-SOT children. Our findings support the need for tailored strategies for these high-risk children.
儿童实体器官移植(SOT)患者发生严重 COVID-19 的风险尚不清楚。我们比较了儿科 SOT 与非 SOT 儿童 COVID-19 严重感染的相对风险。
使用新构建的 K-COV-N 队列(韩国疾病控制与预防机构-COVID-19-国家健康保险服务)。纳入 2008 年 1 月至 2022 年 1 月期间接受 SOT 的 COVID-19 儿童(年龄<18 岁)。使用倾向评分匹配,按 1:4 的比例选择非 SOT COVID-19 儿童。根据需要呼吸支持的情况,建立了三种严重 COVID-19 的定义:严重 I(需要高流量鼻导管或住院时间延长≥6 天以上的呼吸支持)、严重 II(需要任何氧气补充)和严重 III(需要任何氧气补充或住院时间延长≥6 天)。
在 2957323 例 COVID-19 儿童中,纳入 206 例儿科 SOT 受者(SOTR)和 803 例匹配的非 SOT 儿童进行分析。大多数感染(96.6%)发生在奥密克戎流行期间;无死亡病例报告。儿科 SOTR 发生严重 I 的风险高 3.6 倍(95%置信区间:1.1-11.7,P=0.03),发生严重 III 的风险高 4.9 倍(95%置信区间:1.6-15.0,P=0.006),而非 SOT 儿童则无严重 II 型病例。虽然没有统计学意义,但接种疫苗的 SOT 组未报告严重 COVID-19 病例(严重 III 型为 0.0% vs 5.7%,P=0.09)。
儿科 SOTR 发生严重 COVID-19 的风险明显高于非 SOT 儿童。我们的研究结果支持针对这些高危儿童制定个体化策略的必要性。