Universidade Federal do Rio Grande do Sul (UFRGS), Departamento de Pediatria e Programa de Pós-Graduação em Saúde da Criança e do Adolescente (PPGSCA), Porto Alegre, RS, Brazil; Hospital de Clínicas de Porto Alegre, Unidade de Terapia Intensiva Neonatal, Porto Alegre, RS, Brazil.
Hospital de Clínicas de Porto Alegre, Departamento de Educação Física e Terapia Ocupacional, Porto Alegre, RS, Brazil.
J Pediatr (Rio J). 2024 Jan-Feb;100(1):8-24. doi: 10.1016/j.jped.2023.05.008. Epub 2023 Jun 21.
To compare LISA with INSURE technique for surfactant administration in preterm with gestational age (GA) < 36 weeks with RDS in respect to the incidence of pneumothorax, bronchopulmonary dysplasia (BPD), need for mechanical ventilation (MV), regional cerebral oxygen saturation (rSO2), peri‑intraventricular hemorrhage (PIVH) and mortality.
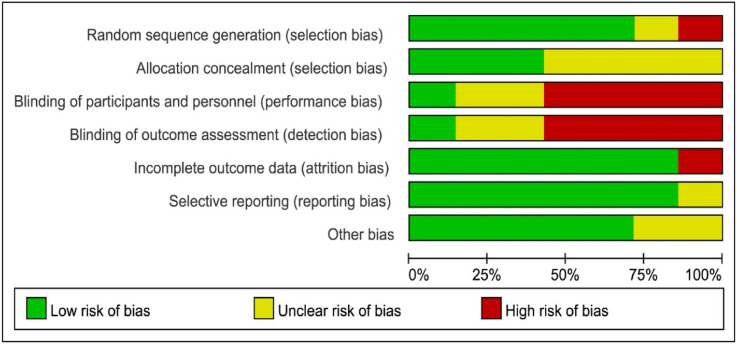
A systematic search in PubMed, Embase, Lilacs, CINAHL, SciELO databases, Brazilian Registry of Randomized Clinical Trials (ReBEC), Clinicaltrials.gov, and Cochrane Central Register of Controlled Trials (CENTRAL) was performed. RCTs evaluating the effects of the LISA technique versus INSURE in preterm infants with gestational age < 36 weeks and that had as outcomes evaluation of the rates of pneumothorax, BPD, need for MV, rSO2, PIVH, and mortality were included in the meta-analysis. Random effects and hazard ratio models were used to combine all study results. Inter-study heterogeneity was assessed using Cochrane Q statistics and Higgin's I2 statistics.
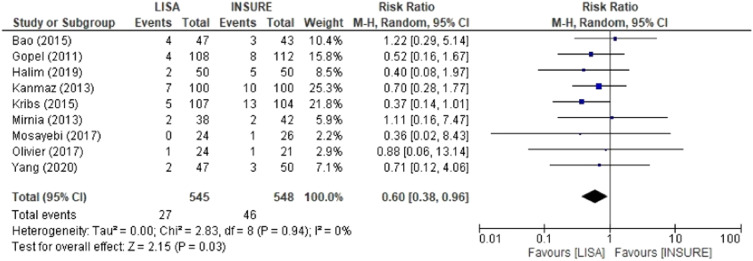
Sixteen RCTs published between 2012 and 2020 met the inclusion criteria, a total of 1,944 preterms. Eleven studies showed a shorter duration of MV and CPAP in the LISA group than in INSURE group. Two studies evaluated rSO2 and suggested that LISA and INSURE transiently affect brain autoregulation during surfactant administration. INSURE group had a higher risk for MV in the first 72 h of life, pneumothorax, PIVH and mortality in comparison to the LISA group.
This systematic review and meta-analyses provided evidence for the benefits of the LISA technique in the treatment of RDS, decreasing CPAP time, need for MV, BPD, pneumothorax, PIVH, and mortality when compared to INSURE.
比较 LISA 与 INSURE 技术在治疗胎龄(GA)<36 周且患有 RDS 的早产儿中的应用,以比较气胸、支气管肺发育不良(BPD)、机械通气(MV)需求、局部脑氧饱和度(rSO2)、室周-脑室内出血(PIVH)和死亡率的发生率。
在 PubMed、Embase、Lilacs、CINAHL、SciELO 数据库、巴西随机临床试验注册处(ReBEC)、Clinicaltrials.gov 和 Cochrane 对照试验中心注册库(CENTRAL)中进行系统检索。纳入了评估 LISA 技术与 INSURE 技术对胎龄<36 周且评估气胸、BPD、MV 需求、rSO2、PIVH 和死亡率发生率的早产儿影响的 RCT 进行荟萃分析。使用随机效应和危害比模型合并所有研究结果。使用 Cochrane Q 统计量和 Higgin's I2 统计量评估研究间异质性。
2012 年至 2020 年期间发表的 16 项 RCT 符合纳入标准,共有 1944 名早产儿。11 项研究表明 LISA 组的 MV 和 CPAP 持续时间比 INSURE 组短。两项研究评估了 rSO2,并表明 LISA 和 INSURE 在给予表面活性剂时会短暂影响脑自动调节。与 LISA 组相比,INSURE 组在生命的前 72 小时内 MV、气胸、PIVH 和死亡率的风险更高。
本系统评价和荟萃分析提供了证据,表明 LISA 技术在治疗 RDS 方面具有优势,与 INSURE 相比,可减少 CPAP 时间、MV、BPD、气胸、PIVH 和死亡率。