Dahiya Dushyant Singh, Jahagirdar Vinay, Chandan Saurabh, Gangwani Manesh Kumar, Merza Nooraldin, Ali Hassam, Deliwala Smit, Aziz Muhammad, Ramai Daryl, Pinnam Bhanu Siva Mohan, Bapaye Jay, Cheng Chin-I, Inamdar Sumant, Sharma Neil R, Al-Haddad Mohammad
Department of Internal Medicine, Central Michigan University College of Medicine, Saginaw, MI 48601, United States.
Department of Internal Medicine, University of Missouri-Kansas City, Kansas City, MO 64110, United States.
World J Hepatol. 2023 Jun 27;15(6):797-812. doi: 10.4254/wjh.v15.i6.797.
Acute pancreatitis (AP) in liver transplant (LT) recipients may lead to poor clinical outcomes and development of severe complications.
We aimed to assess national trends, clinical outcomes, and the healthcare burden of LT hospitalizations with AP in the United States (US).
The National Inpatient Sample was utilized to identify all adult (≥ 18 years old) LT hospitalizations with AP in the US from 2007-2019. Non-LT AP hospitalizations served as controls for comparative analysis. National trends of hospitalization characteristics, clinical outcomes, complications, and healthcare burden for LT hospitalizations with AP were highlighted. Hospitalization characteristics, clinical outcomes, complications, and healthcare burden were also compared between the LT and non-LT cohorts. Furthermore, predictors of inpatient mortality for LT hospitalizations with AP were identified. All values ≤ 0.05 were considered statistically significant.
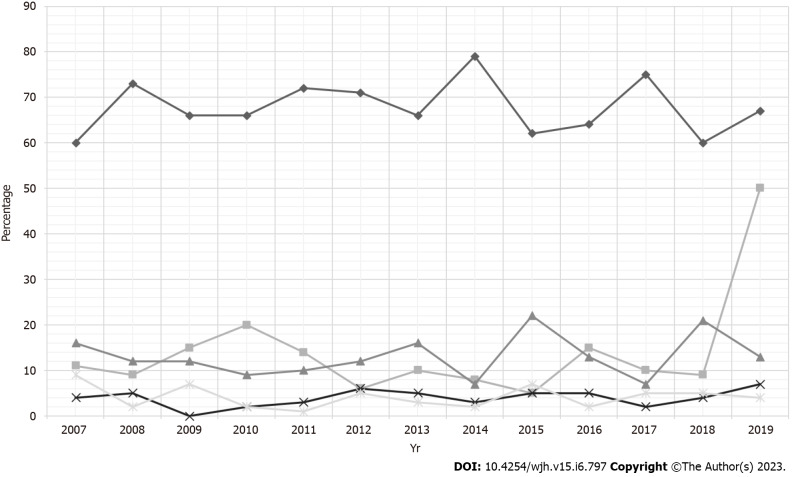
The total number of LT hospitalizations with AP increased from 305 in 2007 to 610 in 2019. There was a rising trend of Hispanic (16.5% in 2007 to 21.1% in 2018, P-trend = 0.0009) and Asian (4.3% in 2007 to 7.4% in 2019, p-trend = 0.0002) LT hospitalizations with AP, while a decline was noted for Blacks (11% in 2007 to 8.3% in 2019, P-trend = 0.0004). Furthermore, LT hospitalizations with AP had an increasing comorbidity burden as the Charlson Comorbidity Index (CCI) score ≥ 3 increased from 41.64% in 2007 to 62.30% in 2019 (P-trend < 0.0001). We did not find statistically significant trends in inpatient mortality, mean length of stay (LOS), and mean total healthcare charge (THC) for LT hospitalizations with AP despite rising trends of complications such as sepsis, acute kidney failure (AKF), acute respiratory failure (ARF), abdominal abscesses, portal vein thrombosis (PVT), and venous thromboembolism (VTE). Between 2007-2019, 6863 LT hospitalizations with AP were compared to 5649980 non-LT AP hospitalizations. LT hospitalizations with AP were slightly older (53.5 52.6 years, = 0.017) and had a higher proportion of patients with CCI ≥ 3 (51.5% 19.8%, < 0.0001) compared to the non-LT cohort. Additionally, LT hospitalizations with AP had a higher proportion of Whites (67.9% 64.6%, < 0.0001) and Asians (4% 2.3%, < 0.0001), while the non-LT cohort had a higher proportion of Blacks and Hispanics. Interestingly, LT hospitalizations with AP had lower inpatient mortality (1.37% 2.16%, = 0.0479) compared to the non-LT cohort despite having a higher mean age, CCI scores, and complications such as AKF, PVT, VTE, and the need for blood transfusion. However, LT hospitalizations with AP had a higher mean THC ($59596 $50466, = 0.0429) than the non-LT cohort.
In the US, LT hospitalizations with AP were on the rise, particularly for Hispanics and Asians. However, LT hospitalizations with AP had lower inpatient mortality compared to non-LT AP hospitalizations.
肝移植(LT)受者发生急性胰腺炎(AP)可能导致不良临床结局及严重并发症的发生。
我们旨在评估美国LT合并AP住院治疗的全国趋势、临床结局及医疗负担。
利用全国住院患者样本确定2007年至2019年美国所有成年(≥18岁)LT合并AP的住院患者。非LT的AP住院患者作为对照进行比较分析。突出了LT合并AP住院患者的住院特征、临床结局、并发症及医疗负担的全国趋势。还比较了LT组和非LT组的住院特征、临床结局、并发症及医疗负担。此外,确定了LT合并AP住院患者的住院死亡率预测因素。所有P值≤0.05被认为具有统计学意义。
LT合并AP的住院患者总数从2007年的305例增加到2019年的610例。LT合并AP的住院患者中,西班牙裔(从2007年的16.5%增至2018年的21.1%,P趋势=0.0009)和亚裔(从2007年的4.3%增至2019年的7.4%,P趋势=0.0002)呈上升趋势,而黑人呈下降趋势(从2007年的11%降至2019年的8.3%,P趋势=0.0004)。此外,随着查尔森合并症指数(CCI)评分≥3的患者比例从2007年的41.64%增至2019年的62.30%(P趋势<0.0001),LT合并AP的住院患者合并症负担增加。尽管脓毒症、急性肾衰竭(AKF)、急性呼吸衰竭(ARF)、腹腔脓肿、门静脉血栓形成(PVT)和静脉血栓栓塞(VTE)等并发症呈上升趋势,但我们未发现LT合并AP住院患者的住院死亡率、平均住院时间(LOS)和平均总医疗费用(THC)有统计学意义的趋势。2007年至2019年期间,6863例LT合并AP的住院患者与5649980例非LT的AP住院患者进行了比较。与非LT组相比,LT合并AP的住院患者年龄稍大(53.5对52.6岁,P=0.017),CCI评分≥3的患者比例更高(51.5%对19.8%,P<0.0001)。此外,LT合并AP的住院患者中白人(67.9%对64.6%,P<0.0001)和亚裔(4%对2.3%,P<0.0001)比例更高,而非LT组中黑人和西班牙裔比例更高。有趣的是,尽管LT合并AP的住院患者平均年龄、CCI评分更高,且有AKF、PVT、VTE等并发症以及输血需求,但与非LT组相比住院死亡率更低(1.37%对2.16%,P=0.0479)。然而,LT合并AP的住院患者平均THC(59596美元对50466美元,P=0.0429)高于非LT组。
在美国,LT合并AP的住院患者数量呈上升趋势,尤其是西班牙裔和亚裔。然而,与非LT的AP住院患者相比,LT合并AP的住院患者住院死亡率更低。