Department of Computer Science, University of Oxford, Oxford, UK.
Department of Cardiology, Oxford University Hospitals NHS Foundation Trust, Oxford, UK.
J Physiol. 2023 Sep;601(18):4013-4032. doi: 10.1113/JP284730. Epub 2023 Jul 20.
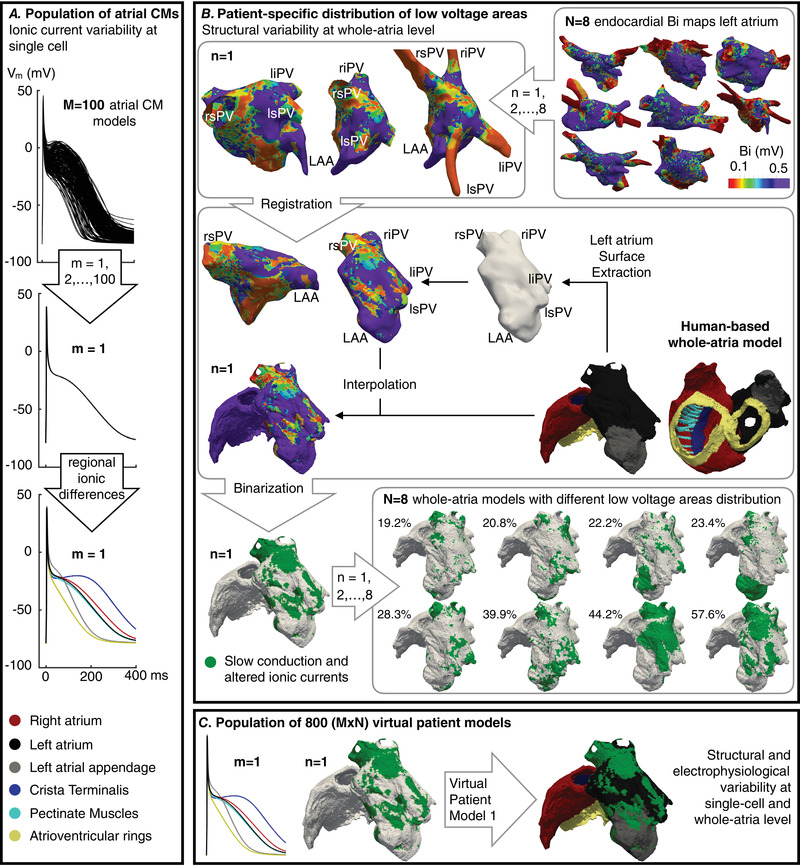
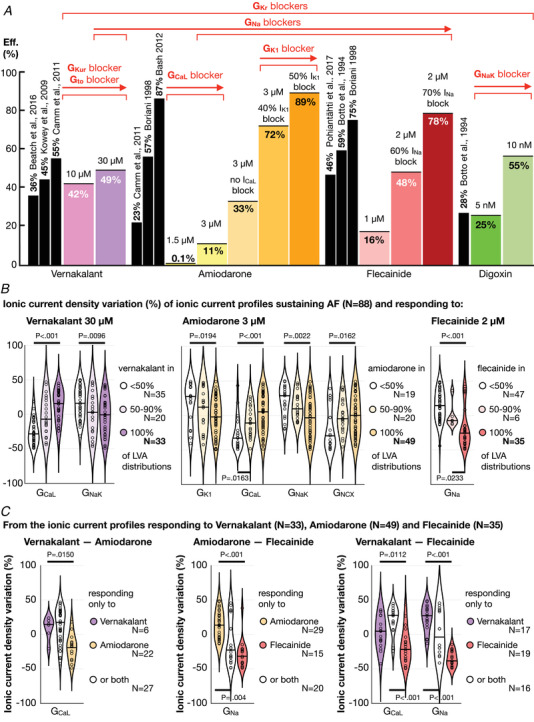
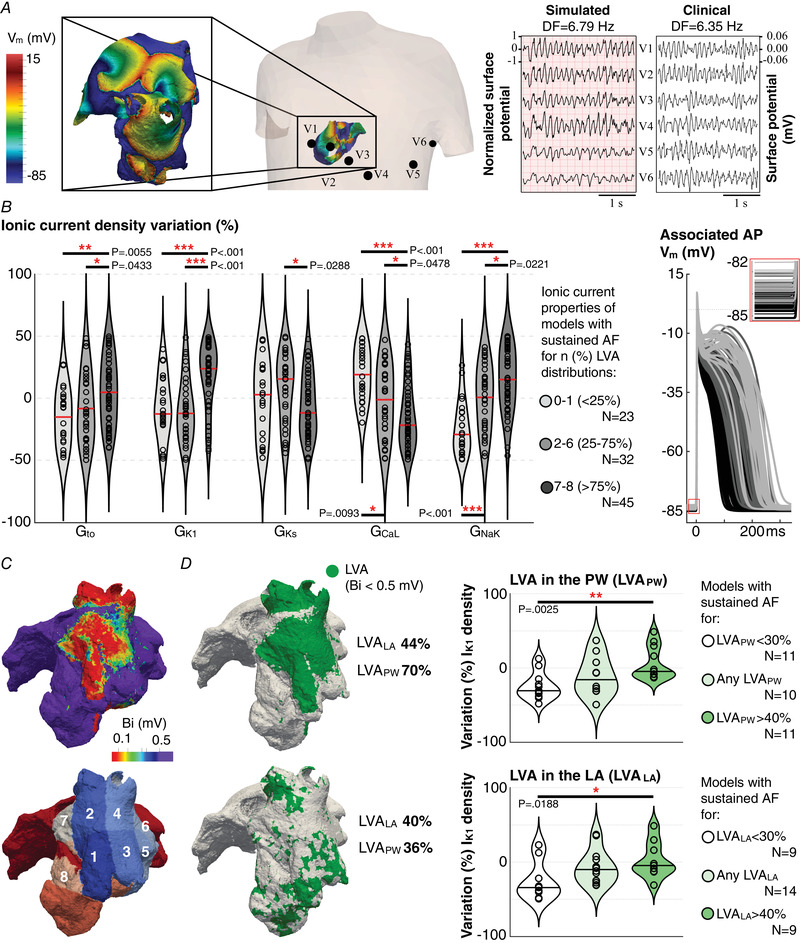
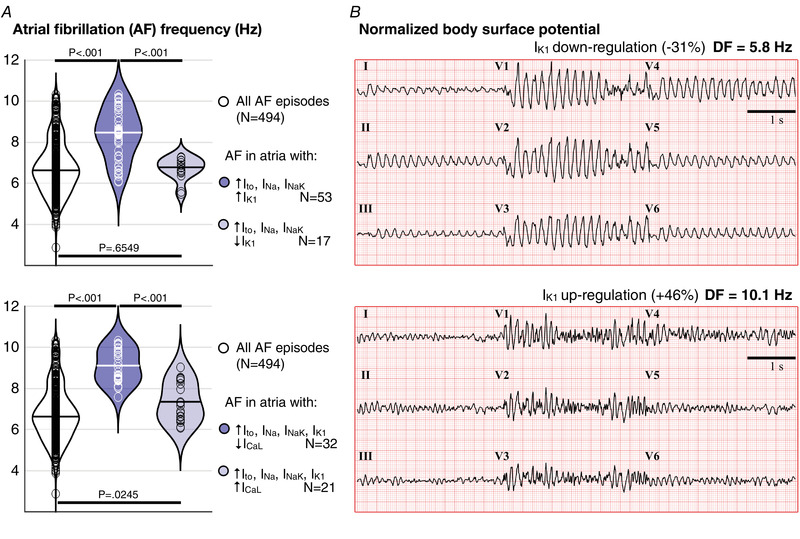
The best pharmacological treatment for each atrial fibrillation (AF) patient is unclear. We aim to exploit AF simulations in 800 virtual atria to identify key patient characteristics that guide the optimal selection of anti-arrhythmic drugs. The virtual cohort considered variability in electrophysiology and low voltage areas (LVA) and was developed and validated against experimental and clinical data from ionic currents to ECG. AF sustained in 494 (62%) atria, with large inward rectifier K current (I ) and Na /K pump (I ) densities (I 0.11 ± 0.03 vs. 0.07 ± 0.03 S mF ; I 0.68 ± 0.15 vs. 0.38 ± 26 S mF ; sustained vs. un-sustained AF). In severely remodelled left atrium, with LVA extensions of more than 40% in the posterior wall, higher I (median density 0.12 ± 0.02 S mF ) was required for AF maintenance, and rotors localized in healthy right atrium. For lower LVA extensions, rotors could also anchor to LVA, in atria presenting short refractoriness (median L-type Ca current, I , density 0.08 ± 0.03 S mF ). This atrial refractoriness, modulated by I and fast Na current (I ), determined pharmacological treatment success for both small and large LVA. Vernakalant was effective in atria presenting long refractoriness (median I density 0.13 ± 0.05 S mF ). For short refractoriness, atria with high I (median density 8.92 ± 2.59 S mF ) responded more favourably to amiodarone than flecainide, and the opposite was found in atria with low I (median density 5.33 ± 1.41 S mF ). In silico drug trials in 800 human atria identify inward currents as critical for optimal stratification of AF patient to pharmacological treatment and, together with the left atrial LVA extension, for accurately phenotyping AF dynamics. KEY POINTS: Atrial fibrillation (AF) maintenance is facilitated by small L-type Ca current (I ) and large inward rectifier K current (I ) and Na /K pump. In severely remodelled left atrium, with low voltage areas (LVA) covering more than 40% of the posterior wall, sustained AF requires higher I and rotors localize in healthy right atrium. For lower LVA extensions, rotors can also anchor to LVA, if the atria present short refractoriness (low I ) Vernakalant is effective in atria presenting long refractoriness (high I ). For short refractoriness, atria with fast Na current (I ) up-regulation respond more favourably to amiodarone than flecainide, and the opposite is found in atria with low I . The inward currents (I and I ) are critical for optimal stratification of AF patient to pharmacological treatment and, together with the left atrial LVA extension, for accurately phenotyping AF dynamics.
对于每个心房颤动(AF)患者,最佳的药理学治疗方法尚不清楚。我们旨在利用 800 个虚拟心房中的 AF 模拟来确定关键的患者特征,以指导抗心律失常药物的最佳选择。虚拟队列考虑了电生理学和低电压区(LVA)的变异性,并针对离子电流到心电图的实验和临床数据进行了开发和验证。494 个(62%)心房中持续发生 AF,具有较大的内向整流钾电流(I )和 Na / K 泵(I )密度(I 0.11 ± 0.03 对 0.07 ± 0.03 S mF ; I 0.68 ± 0.15 对 0.38 ± 26 S mF ;持续与非持续 AF)。在严重重塑的左心房中,如果后侧壁的 LVA 扩展超过 40%,则需要更高的 I (中位数密度 0.12 ± 0.02 S mF )来维持 AF,并且转子定位于健康的右心房中。对于较低的 LVA 扩展,如果心房呈现较短的不应期(中位数 L 型 Ca 电流,I ,密度 0.08 ± 0.03 S mF ),则转子也可以锚定在 LVA 上。由 I 和快速 Na 电流(I )调制的这种心房不应期决定了 LVA 大小对药物治疗的成功。维纳卡兰在呈现长不应期(中位数 I 密度 0.13 ± 0.05 S mF )的心房中有效。对于较短的不应期,具有较高 I (中位数密度 8.92 ± 2.59 S mF )的心房对胺碘酮的反应比氟卡尼更有利,而在具有较低 I (中位数密度 5.33 ± 1.41 S mF )的心房中则相反。在 800 个人类心房的计算机药物试验中,内向电流被确定为 AF 患者药物治疗分层的关键,并与左心房 LVA 扩展一起,用于准确表型化 AF 动力学。
小的 L 型 Ca 电流(I )和大的内向整流钾电流(I )和 Na / K 泵促进 AF 的维持。在严重重塑的左心房中,如果 LVA 覆盖后侧壁超过 40%,持续的 AF 需要更高的 I ,并且转子定位于健康的右心房中。对于较低的 LVA 扩展,如果心房呈现较短的不应期(低 I ),则转子也可以锚定在 LVA 上。维纳卡兰在呈现长不应期(高 I )的心房中有效。对于较短的不应期,具有快速 Na 电流(I )上调的心房对胺碘酮的反应比氟卡尼更有利,而在具有低 I )的心房中则相反。内向电流(I 和 I )对于 AF 患者药物治疗的最佳分层以及与左心房 LVA 扩展一起用于准确表型化 AF 动力学至关重要。