Agarwal Dinesh K, Mulholland Clancy, Koye Digsu N, Sathianathen Niranjan, Yao Henry, Dundee Philip, Moon Daniel, Furrer Marc, Giudice Christina, Wang Wayland, Simpson Julie A, Kearsley Jamie, Norris Briony, Zargar Homi, Pan Henry Y C, Agarwal Ashwin, Lawrentschuk Nathan, Corcoran Niall M
Department of Urology, The Royal Melbourne Hospital, Melbourne, Australia.
Department of Urology, Western Health, Melbourne, Australia.
Eur Urol Open Sci. 2023 Jun 15;54:33-42. doi: 10.1016/j.euros.2023.05.007. eCollection 2023 Aug.
The surgical difficulty of partial nephrectomy (PN) varies depending on the operative approach. Existing nephrometry classifications for assessment of surgical difficulty are not specific to the robotic approach.
To develop an international robotic-specific classification of renal masses for preoperative assessment of surgical difficulty of robotic PN.
The RPN classification (Radius, Position of tumour, iNvasion of renal sinus) considers three parameters: tumour size, tumour position, and invasion of the renal sinus. In an international survey, 45 experienced robotic surgeons independently reviewed de-identified computed tomography images of 144 patients with renal tumours to assess surgical difficulty of robot-assisted PN using a 10-point Likert scale. A separate data set of 248 patients was used for external validation.
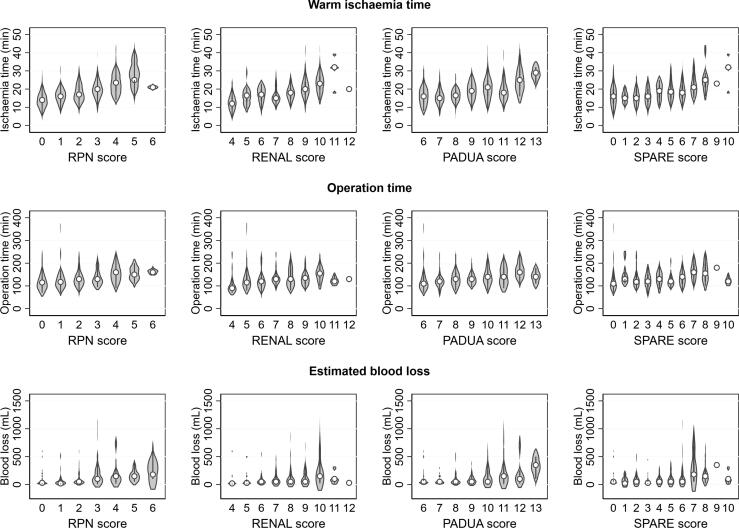
Multiple linear regression was conducted and a risk score was developed after rounding the regression coefficients. The RPN classification was correlated with the surgical difficulty score derived from the international survey. External validation was performed using a retrospective cohort of 248 patients. RPN classification was also compared with the RENAL (Radius; Exophytic/endophytic; Nearness; Anterior/posterior; Location), PADUA (Preoperative Aspects and Dimensions Used for Anatomic), and SPARE (Simplified PADUA REnal) scoring systems.
The median tumour size was 38 mm (interquartile range 27-49). The majority (81%) of renal tumours were peripheral, followed by hilar (12%) and central (7.6%) locations. Noninvasive and semi-invasive tumours accounted for 37% each, and 26% of the tumours were invasive. The mean surgical difficulty score was 5.2 (standard deviation 1.9). Linear regression analysis indicated that the RPN classification correlated very well with the surgical difficulty score (R = 0.80). The R values for the other scoring systems were: 0.66 for RENAL, 0.75 for PADUA, and 0.70 for SPARE. In an external validation cohort, the performance of all four classification systems in predicting perioperative outcomes was similar, with low R values.
The proposed RPN classification is the first nephrometry system to assess the surgical difficulty of renal masses for which robot-assisted PN is planned, and is a useful tool to assist in surgical planning, training and data reporting.
We describe a simple classification system to help urologists in preoperative assessment of the difficulty of robotic surgery for partial kidney removal for kidney tumours.
部分肾切除术(PN)的手术难度因手术入路而异。现有的用于评估手术难度的肾计量分类并不针对机器人手术入路。
制定一种国际上特定于机器人手术的肾肿块分类方法,用于术前评估机器人辅助PN的手术难度。
设计、设置和参与者:RPN分类(半径、肿瘤位置、肾窦侵犯情况)考虑三个参数:肿瘤大小、肿瘤位置和肾窦侵犯情况。在一项国际调查中,45名经验丰富的机器人外科医生独立审查了144例肾肿瘤患者的去识别计算机断层扫描图像,使用10分李克特量表评估机器人辅助PN的手术难度。另外一组248例患者的数据集用于外部验证。
进行多元线性回归,并在对回归系数进行四舍五入后制定风险评分。RPN分类与国际调查得出的手术难度评分相关。使用248例患者的回顾性队列进行外部验证。还将RPN分类与RENAL(半径;外生性/内生性;接近度;前/后;位置)、PADUA(用于解剖的术前方面和尺寸)和SPARE(简化的PADUA肾)评分系统进行比较。
肿瘤大小的中位数为38mm(四分位间距27 - 49)。大多数(81%)肾肿瘤位于周边,其次是肾门(12%)和中央(7.6%)位置。非侵袭性和半侵袭性肿瘤各占37%,26%的肿瘤为侵袭性。平均手术难度评分为5.2(标准差1.9)。线性回归分析表明,RPN分类与手术难度评分相关性非常好(R = 0.80)。其他评分系统的R值分别为:RENAL为0.66,PADUA为0.75,SPARE为0.70。在外部验证队列中,所有四种分类系统在预测围手术期结果方面的表现相似,R值较低。
所提出的RPN分类是第一个用于评估计划进行机器人辅助PN的肾肿块手术难度的肾计量系统,是协助手术规划、培训和数据报告的有用工具。
我们描述了一种简单的分类系统,以帮助泌尿科医生在术前评估针对肾肿瘤进行部分肾切除的机器人手术的难度。