Department of Psychiatry, Queen's University, Kingston, ON, Canada.
Centre for Neuroscience Studies, Queen's University, Kingston, ON, Canada.
Can J Psychiatry. 2023 Aug;68(8):605-612. doi: 10.1177/07067437231156235. Epub 2023 Feb 21.
There is limited data about the impact of mood disorders treatment guidelines on clinical outcomes. The objective of this study was to investigate the impact of prescribers' adherence to the 2018 Canadian Network for Mood and Anxiety Treatments (CANMAT) and International Society for Bipolar Disorders (ISBD) treatment guidelines recommendations on the readmission rates of patients hospitalized for mania.
A retrospective cohort of all individuals admitted due to acute mania to Kingston General Hospital, Kingston, ON, from January 2018 to July 2021 was included in this study. Patient variables and data regarding index admission and subsequent hospitalizations were extracted from medical records up to December 31, 2021. Treatment regimens were classified as first-line, second-line, noncompliant, or no treatment. We explored the associations between treatment regimens and the risk of readmissions using univariate, multivariate, and survival analysis.
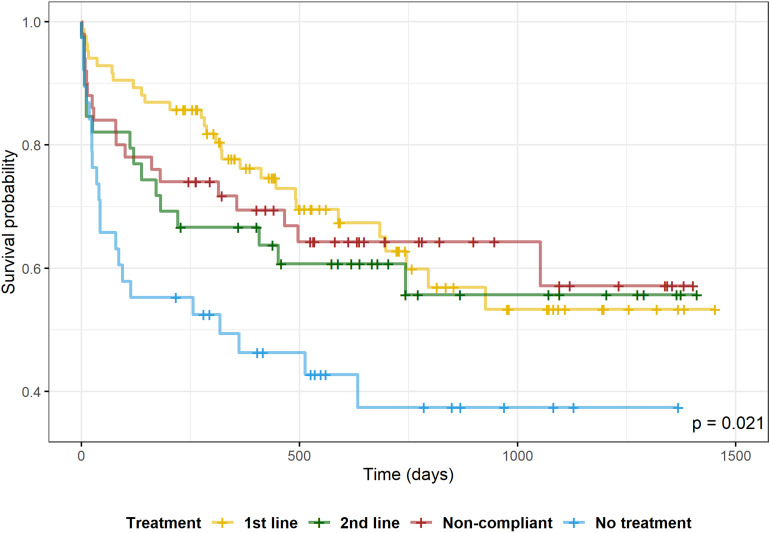
We identified 211 hospitalizations related to 165 patients. The mean time-to-readmission was 211.8 days (standard deviation [SD] = 247.1); the 30-day rehospitalization rate was 13.7%, and any rehospitalization rate was 40.3%. Compared to no treatment, only first-line treatments were associated with a statistically significant decreased risk of 30-day readmission (odds ratio [OR] = 0.209; 95% CI, 0.058 to 0.670). The risk of any readmission was reduced by first-line (OR = 0.387; 95% CI, 0.173 to 0.848) and noncompliant regimens (OR = 0.414; 95% CI, 0.174 to 0.982) compared to no treatment. On survival analysis, no treatment group was associated with shorter time-to-readmission (log-rank test, = 0.014) and increased risk of readmission (hazard ratio = 2.27; 95% CI, 1.30 to 3.96) when compared to first-line medications.
Treatment with first-line medications was associated with lower 30-day rehospitalization rates and longer time-to-readmission. Physicians' adherence to treatments with higher-ranked evidence for efficacy, safety, and tolerability may improve bipolar disorder outcomes.
关于心境障碍治疗指南对临床结局影响的数据有限。本研究的目的是调查遵循 2018 年加拿大心境与焦虑治疗网络(CANMAT)和国际双相障碍学会(ISBD)治疗指南建议的医生对因躁狂住院患者的再入院率的影响。
本研究纳入了 2018 年 1 月至 2021 年 7 月期间因急性躁狂症入住金斯顿总医院的所有患者。从病历中提取患者变量以及索引入院和随后住院的数据,直至 2021 年 12 月 31 日。治疗方案分为一线、二线、不符合或无治疗。我们使用单变量、多变量和生存分析来探讨治疗方案与再入院风险之间的关联。
我们确定了 165 名患者的 211 次住院。中位再入院时间为 211.8 天(标准差[SD] = 247.1);30 天再入院率为 13.7%,任何再入院率为 40.3%。与无治疗相比,只有一线治疗与 30 天再入院的风险显著降低相关(优势比[OR] = 0.209;95%置信区间,0.058 至 0.670)。与无治疗相比,一线治疗(OR = 0.387;95%置信区间,0.173 至 0.848)和不符合治疗方案(OR = 0.414;95%置信区间,0.174 至 0.982)的风险降低。在生存分析中,与一线药物相比,无治疗组再入院时间更短(对数秩检验,P = 0.014),再入院风险更高(风险比[HR] = 2.27;95%置信区间,1.30 至 3.96)。
一线药物治疗与较低的 30 天再入院率和较长的再入院时间相关。医生遵循具有更高疗效、安全性和耐受性证据的治疗方法可能会改善双相情感障碍的结局。