Queen Elizabeth Hospital, University Hospitals Birmingham NHS Foundation Trust, UK.
Institute of Cancer and Genomic Sciences, University of Birmingham, UK.
Ann R Coll Surg Engl. 2024 Apr;106(4):369-376. doi: 10.1308/rcsann.2022.0140. Epub 2023 Aug 29.
Staging laparoscopy (SL) has become commonplace in the preoperative staging pathway for oesophagogastric (OG) cancer. SL is often performed before curative treatment to examine for macroscopic peritoneal metastases (PM) or positive peritoneal cytology (PPC). The aim of this study was to develop an objective risk scoring system to predict both PM and PPC at SL.
A prospectively collected and maintained database of all OG cancer patients treated between 2006 and 2020 was reviewed. Univariate and multivariate analyses were performed to identify risk factors for both PM and PPC at SL. A risk score was produced for both PM and PPC, and then validated internally.
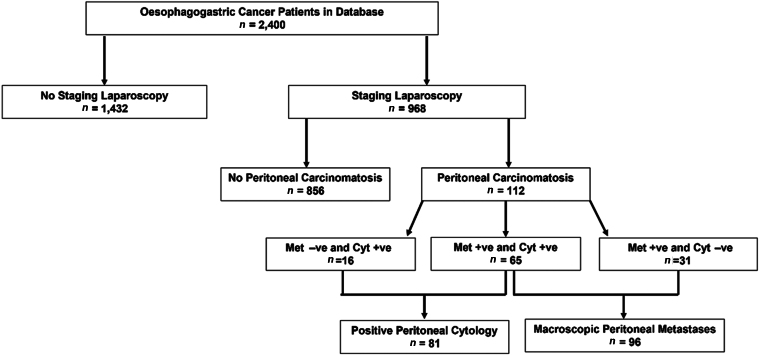
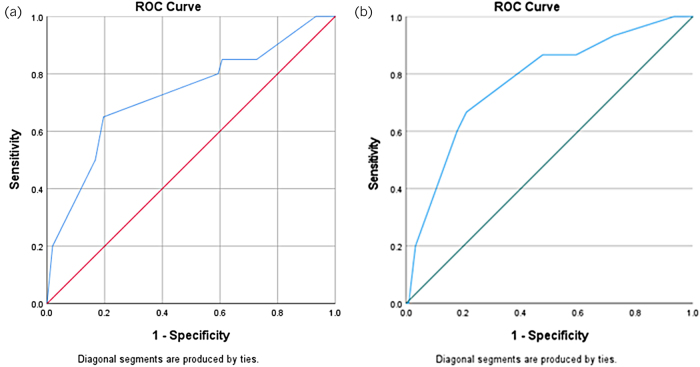
Among 968 patients who underwent SL, 96 (9.9%) had PM and 81 (8.4%) had PPC at SL. Tumour site ( < 0.001), computed tomography (CT) T stage ( < 0.001) and N stage ( = 0.029) were significantly associated with PM at SL ( < 0.001). Tumour site ( < 0.001), biopsy histology ( = 0.041), CT T stage ( < 0.001) and N stage ( < 0.001) were significantly associated with PPC. The risk scoring model for PM included cancer site and CT T stage. This was successfully tested on the validation set (area under the receiver operating characteristic [AUROC] = 0.730). The risk scoring model for PPC included cancer site, CT T and N stage. This was successfully tested on the validation set (AUROC = 0.773).
The current risk scores are valid tools with which to predict the risk PM and PPC in patients undergoing SL for OG cancer and may help to avoid subjecting patients to unnecessary SL.
腹腔镜分期(SL)已成为食管胃(OG)癌术前分期途径中的常规手段。SL 通常在进行治愈性治疗之前进行,以检查是否存在肉眼可见的腹膜转移(PM)或阳性腹膜细胞学(PPC)。本研究旨在开发一种客观的风险评分系统,以预测 SL 时的 PM 和 PPC。
回顾性分析了 2006 年至 2020 年间所有接受 OG 癌症治疗的患者的前瞻性收集和维护数据库。进行单因素和多因素分析,以确定 SL 时 PM 和 PPC 的危险因素。为 PM 和 PPC 生成风险评分,并在内部进行验证。
在 968 例行 SL 的患者中,96 例(9.9%)在 SL 时存在 PM,81 例(8.4%)存在 PPC。肿瘤部位(<0.001)、计算机断层扫描(CT)T 分期(<0.001)和 N 分期(=0.029)与 SL 时的 PM 显著相关(<0.001)。肿瘤部位(<0.001)、活检组织学(=0.041)、CT T 分期(<0.001)和 N 分期(<0.001)与 PPC 显著相关。PM 的风险评分模型包括癌症部位和 CT T 分期。该模型在验证集上成功进行了测试(接受者操作特征曲线下面积 [AUROC] = 0.730)。PPC 的风险评分模型包括癌症部位、CT T 和 N 分期。该模型在验证集上成功进行了测试(AUROC = 0.773)。
目前的风险评分是预测 OG 癌患者接受 SL 时 PM 和 PPC 风险的有效工具,可能有助于避免对患者进行不必要的 SL。