Department of Surgery, Center for Translational Injury Research, McGovern Medical School, The University of Texas Health Science Center at Houston, Houston, Texas.
Shock. 2023 Nov 1;60(5):637-645. doi: 10.1097/SHK.0000000000002216. Epub 2023 Aug 26.
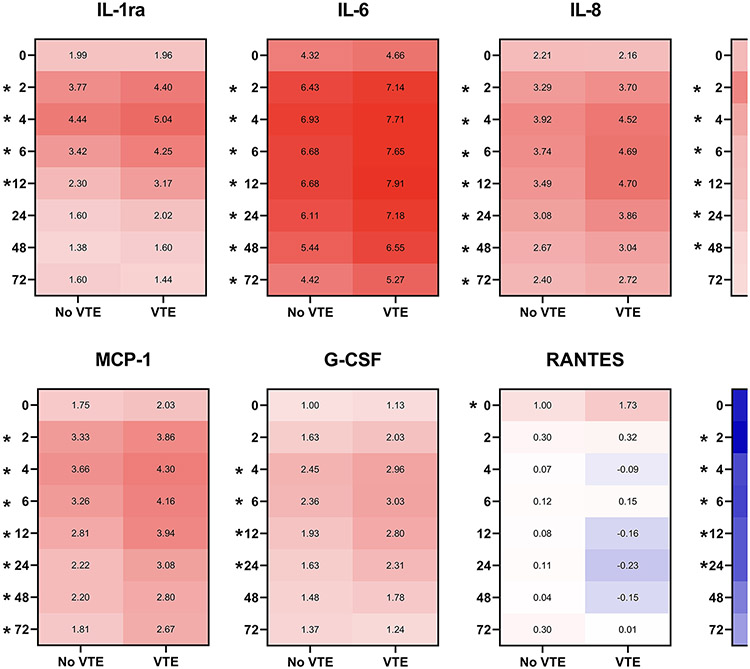
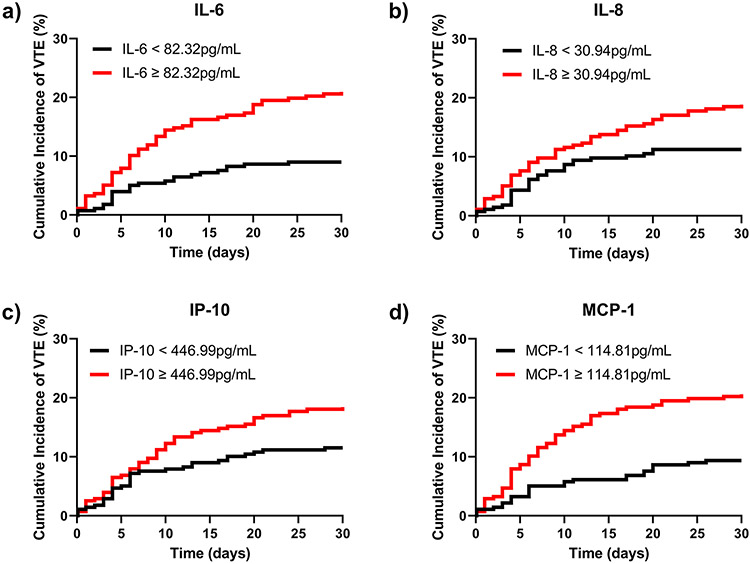
Background: Tissue trauma and hemorrhage result in pronounced activation of the innate immune system. Given known crosstalk between inflammation and coagulation, soluble inflammatory mediators could be associated with venous thromboembolisms (VTEs) after major trauma. Objectives : This study aimed to identify plasma inflammatory mediators that are independent predictors of VTE risk in trauma patients. Methods: We performed a secondary analysis of the Pragmatic Randomized Optimal Platelets and Plasma Ratios (PROPPR) study. Plasma levels of 27 cytokines/chemokines were measured by Bio-Plex at admission and 2, 4, 6, 12, 24, 48, and 72 h later. Patients who died from exsanguination or within 24 h were excluded. Mann-Whitney tests were performed to assess no-VTE and VTE groups at each time point. Multivariable logistic regression was used to determine the adjusted effects of inflammatory mediators on VTE risk. Results: Eighty-six of the 575 patients (15%) included developed VTE. Interleukin (IL)-1ra, IL-6, IL-8, IL-10, eotaxin, granulocyte colony-stimulating factor, interferon-γ-inducible protein, monocyte chemoattractant protein 1 (MCP-1), and chemokine ligand 5 (regulated on activation, normal T cell expressed and secreted) were all significantly increased among VTE patients. Multivariable analyses demonstrated that IL-6, IL-8, interferon-γ-inducible protein, and MCP-1 were independently associated with VTE. Cox proportional hazards modeling identified IL-6, IL-8, and MCP-1 as independent predictors of accelerated VTE development. We identified significant correlations between inflammation and markers of coagulation and endothelial activation. Conclusion: Sustained systemic inflammation is a key driver of VTE risk after major trauma. Therapeutics targeting innate immune activation should be considered for development of future multimodal strategies to augment current VTE prophylaxis.
组织创伤和出血会导致固有免疫系统的显著激活。鉴于炎症和凝血之间存在已知的相互作用,可溶性炎症介质可能与重大创伤后静脉血栓栓塞(VTE)有关。
本研究旨在确定与创伤患者 VTE 风险相关的独立预测因子的血浆炎症介质。
我们对 Pragmatic Randomized Optimal Platelets and Plasma Ratios(PROPPR)研究进行了二次分析。通过 Bio-Plex 在入院时和之后的 2、4、6、12、24、48 和 72 小时测量 27 种细胞因子/趋化因子的血浆水平。排除因出血或 24 小时内死亡的患者。在每个时间点,通过 Mann-Whitney 检验评估无 VTE 和 VTE 组。使用多变量逻辑回归确定炎症介质对 VTE 风险的调整影响。
575 例患者中有 86 例(15%)发生 VTE。白细胞介素(IL)-1ra、IL-6、IL-8、IL-10、嗜酸性粒细胞趋化因子、粒细胞集落刺激因子、干扰素-γ诱导蛋白、单核细胞趋化蛋白 1(MCP-1)和趋化因子配体 5(在激活时调节,正常 T 细胞表达和分泌)在 VTE 患者中均显著升高。多变量分析表明,IL-6、IL-8、干扰素-γ诱导蛋白和 MCP-1 与 VTE 独立相关。Cox 比例风险模型确定 IL-6、IL-8 和 MCP-1 是加速 VTE 发展的独立预测因子。我们发现炎症与凝血和内皮激活标志物之间存在显著相关性。
持续的全身炎症是重大创伤后 VTE 风险的关键驱动因素。针对固有免疫激活的治疗方法应被视为开发未来多模式策略的候选药物,以增强当前的 VTE 预防。