Magenau John, Jaglowski Samantha, Uberti Joseph, Farag Sherif S, Riwes Mary Mansour, Pawarode Attaphol, Anand Sarah, Ghosh Monalisa, Maciejewski John, Braun Thomas, Devenport Martin, Lu Susan, Banerjee Bhramori, DaSilva Carolyn, Devine Steven, Zhang Mei-Jie, Burns Linda J, Liu Yang, Zheng Pan, Reddy Pavan
Transplantation and Cellular Therapy Program, Rogel Cancer Center, University of Michigan, Ann Arbor, MI.
The James Cancer Hospital and Solove Research Institute, Ohio State University, Columbus, OH.
Blood. 2024 Jan 4;143(1):21-31. doi: 10.1182/blood.2023020250.
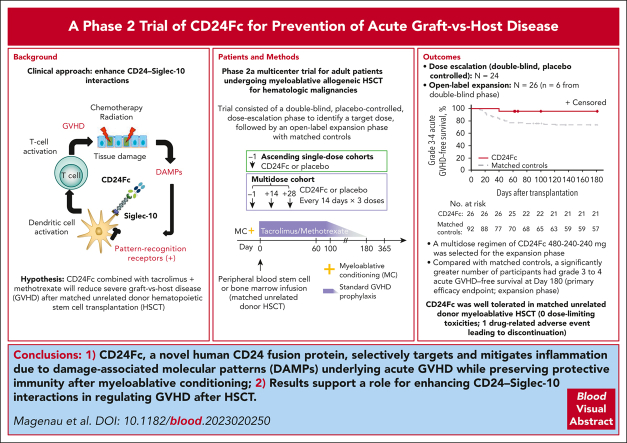
Patients who undergo human leukocyte antigen-matched unrelated donor (MUD) allogeneic hematopoietic stem cell transplantation (HSCT) with myeloablative conditioning for hematologic malignancies often develop acute graft-versus-host disease (GVHD) despite standard calcineurin inhibitor-based prophylaxis in combination with methotrexate. This trial evaluated a novel human CD24 fusion protein (CD24Fc/MK-7110) that selectively targets and mitigates inflammation due to damage-associated molecular patterns underlying acute GVHD while preserving protective immunity after myeloablative conditioning. This phase 2a, multicenter study evaluated the pharmacokinetics, safety, and efficacy of CD24Fc in combination with tacrolimus and methotrexate in preventing acute GVHD in adults undergoing MUD HSCT for hematologic malignancies. A double-blind, placebo-controlled, dose-escalation phase to identify a recommended dose was followed by an open-label expansion phase with matched controls to further evaluate the efficacy and safety of CD24Fc in preventing acute GVHD. A multidose regimen of CD24Fc produced sustained drug exposure with similar safety outcomes when compared with single-dose regimens. Grade 3 to 4 acute GVHD-free survival at day 180 was 96.2% (95% confidence interval [CI], 75.7-99.4) in the CD24Fc expansion cohort (CD24Fc multidose), compared with 73.6% (95% CI, 63.2-81.4) in matched controls (hazard ratio, 0.1 [95% CI, 0.0-0.6]; log-rank test, P = .03). No participants in the CD24Fc escalation or expansion phases experienced dose-limiting toxicities (DLTs). The multidose regimen of CD24Fc was well tolerated with no DLTs and was associated with high rates of severe acute GVHD-free survival after myeloablative MUD HSCT. This trial was registered at ClinicalTrials.gov as #NCT02663622.
接受人白细胞抗原匹配的无关供体(MUD)异基因造血干细胞移植(HSCT)并采用清髓性预处理治疗血液系统恶性肿瘤的患者,尽管采用了基于钙调神经磷酸酶抑制剂并联合甲氨蝶呤的标准预防措施,但仍常发生急性移植物抗宿主病(GVHD)。本试验评估了一种新型人CD24融合蛋白(CD24Fc/MK-7110),该蛋白可选择性靶向并减轻急性GVHD潜在的与损伤相关分子模式引起的炎症,同时在清髓性预处理后保留保护性免疫。这项2a期多中心研究评估了CD24Fc联合他克莫司和甲氨蝶呤在预防接受MUD HSCT治疗血液系统恶性肿瘤的成人急性GVHD方面的药代动力学、安全性和疗效。在一个双盲、安慰剂对照、剂量递增阶段确定推荐剂量后,进行了一个开放标签扩展阶段并设置匹配对照,以进一步评估CD24Fc预防急性GVHD的疗效和安全性。与单剂量方案相比,CD24Fc的多剂量方案产生了持续的药物暴露,且安全性结果相似。在CD24Fc扩展队列(CD24Fc多剂量)中,第180天3至4级无急性GVHD生存率为96.2%(95%置信区间[CI],75.7-99.4),而匹配对照为73.6%(95%CI,63.2-81.‘4)(风险比,0.1[95%CI,0.0-0.6];对数秩检验,P = 0.03)。在CD24Fc剂量递增或扩展阶段,没有参与者出现剂量限制性毒性(DLT)。CD24Fc多剂量方案耐受性良好,无DLT,且与清髓性MUD HSCT后严重无急性GVHD生存率高相关。本试验在ClinicalTrials.gov注册,注册号为#NCT02663622。