Department of Cardiology, Aoyang Hospital Affiliated to Jiangsu University, Zhangjiagang, 215600, China.
Heart Vessels. 2023 Dec;38(12):1431-1441. doi: 10.1007/s00380-023-02314-0. Epub 2023 Sep 25.
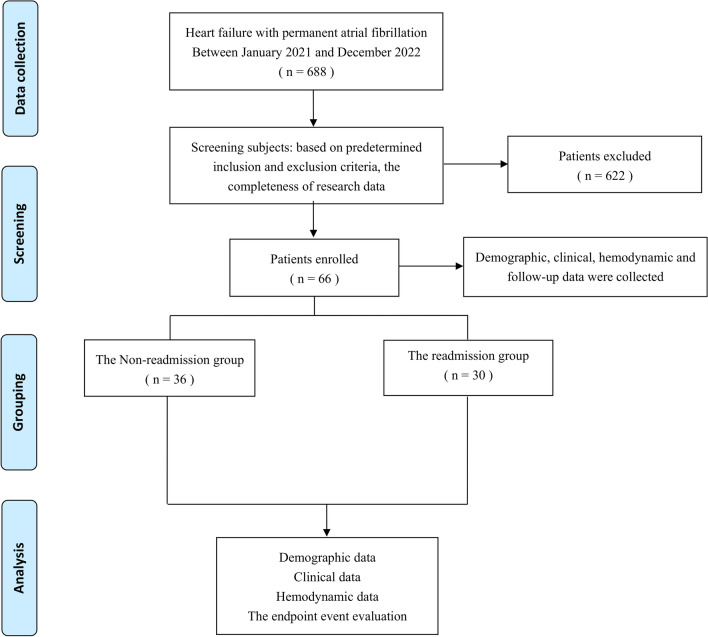
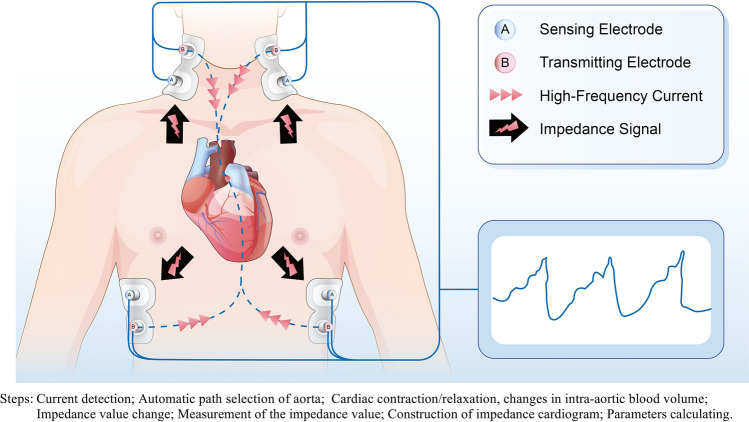
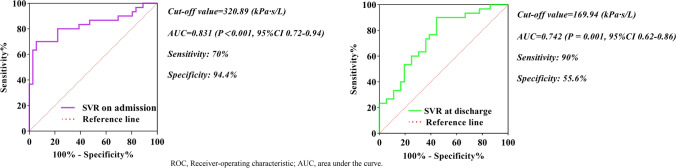
Heart failure (HF) and permanent atrial fibrillation (AF) interact mutually, exacerbating hemodynamic effects and causing adverse outcomes and increased healthcare costs. Monitoring hemodynamic indicators in patients with these comorbidities is crucial for effective clinical management. Transthoracic impedance cardiography (ICG) has been widely employed in assessing hemodynamic status in clinical settings. Given the limited research on the prognostic significance of ICG parameters in HF with permanent AF, we undertook this study. A total of 66 HF patients with permanent AF were included in this retrospective study, and the primary outcome was rehospitalization due to worsening HF within 180-day post-discharge. Cox regression analysis was performed to explore the connection between ICG-evaluated parameters and the outcome risk. Receiver operating characteristic (ROC) curve analysis determined the optimal cutoff values of risk factors, subsequently applied in plotting Kaplan Meier (KM) survival curves. Multivariate Cox regression analysis revealed that systemic vascular resistance (SVR) both on admission and at discharge independently predicted rehospitalization for worsening HF. ROC analysis established optimal SVR cutoff values: 320.89 (kPa s/L) on admission and 169.94 (kPa s/L) at discharge (sensitivity 70%, specificity 94.4%, area under the curve (AUC) 0.831, respectively, sensitivity 90%, specificity 55.6%, AUC 0.742). KM survival curves analysis showed that patients with SVR > 320.89 (kPa s/L) on admission had an 8.14-fold (P < 0.001) increased risk of the end-point event compared with those with SVR ≤ 320.89 (kPa s/L). Similarly, patients with SVR > 169.94 (kPa s/L) at discharge faced a risk elevated by 6.57 times (P = 0.002) relative to those with SVR ≤ 169.94 (kPa s/L). In HF patients with permanent AF, SVR measured by ICG emerges as an independent risk factor and clinical predictor for HF deterioration-related readmission within 180 days after discharge. Higher SVR levels, both upon admission and at discharge, correlate with an incremental rehospitalization risk.
心力衰竭(HF)和永久性心房颤动(AF)相互作用,加重血液动力学效应,导致不良后果和增加医疗保健成本。监测这些合并症患者的血液动力学指标对于有效的临床管理至关重要。经胸阻抗心动图(ICG)已广泛应用于临床评估血液动力学状态。鉴于在永久性 AF 的 HF 中 ICG 参数的预后意义的研究有限,我们进行了这项研究。这项回顾性研究共纳入了 66 例 HF 合并永久性 AF 的患者,主要结局是出院后 180 天内因 HF 恶化而再次住院。采用 Cox 回归分析探讨 ICG 评估参数与结局风险之间的关系。受试者工作特征(ROC)曲线分析确定危险因素的最佳截断值,随后用于绘制 Kaplan-Meier(KM)生存曲线。多变量 Cox 回归分析显示,入院时和出院时的全身血管阻力(SVR)均独立预测因 HF 恶化而再次住院。ROC 分析确定了最佳 SVR 截断值:入院时为 320.89(kPa s/L),出院时为 169.94(kPa s/L)(敏感性 70%,特异性 94.4%,曲线下面积(AUC)为 0.831,敏感性 90%,特异性 55.6%,AUC 为 0.742)。KM 生存曲线分析显示,入院时 SVR > 320.89(kPa s/L)的患者与 SVR ≤ 320.89(kPa s/L)的患者相比,终点事件的风险增加了 8.14 倍(P < 0.001)。同样,出院时 SVR > 169.94(kPa s/L)的患者与 SVR ≤ 169.94(kPa s/L)的患者相比,风险增加了 6.57 倍(P = 0.002)。在 HF 合并永久性 AF 的患者中,ICG 测量的 SVR 是出院后 180 天内 HF 恶化相关再入院的独立危险因素和临床预测因素。入院时和出院时较高的 SVR 水平与再入院风险增加相关。