Sá Couto David, Alexandre André, Costa Ricardo, Campinas Andreia, Santos Mariana, Ribeiro Diana, Torres Severo, Luz André
Cardiology Department, Centro Hospitalar Universitário de Santo António, Largo do Prof. Abel Salazar, 4099-001 Porto, Portugal.
ICBAS School of Medicine and Biomedical Sciences, University of Porto, Rua Jorge Viterbo Ferreira 228, 4050-313 Porto, Portugal.
J Cardiovasc Dev Dis. 2023 Sep 1;10(9):374. doi: 10.3390/jcdd10090374.
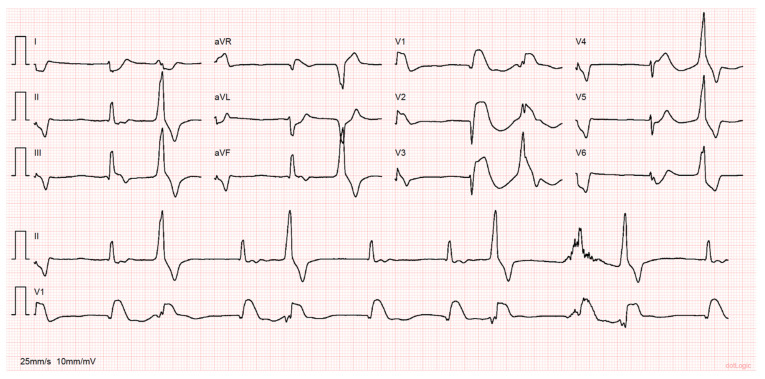
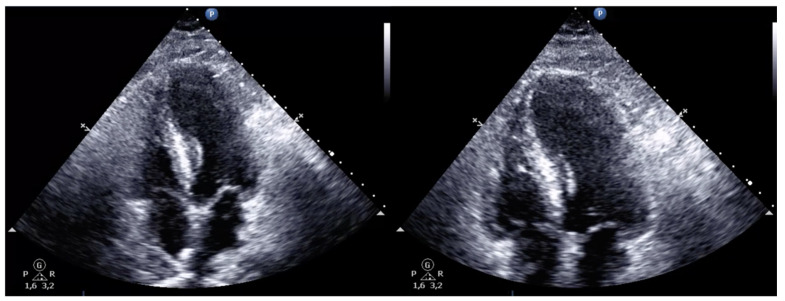
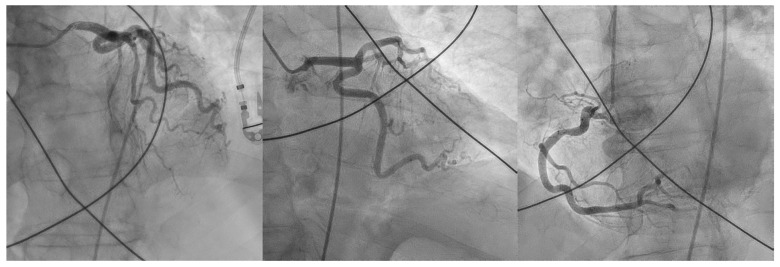
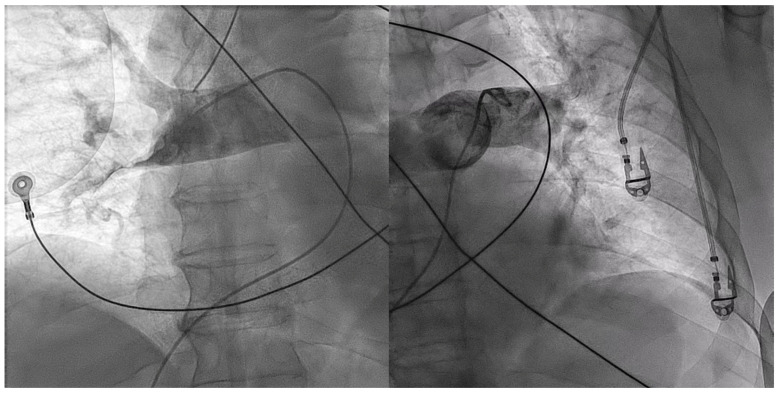
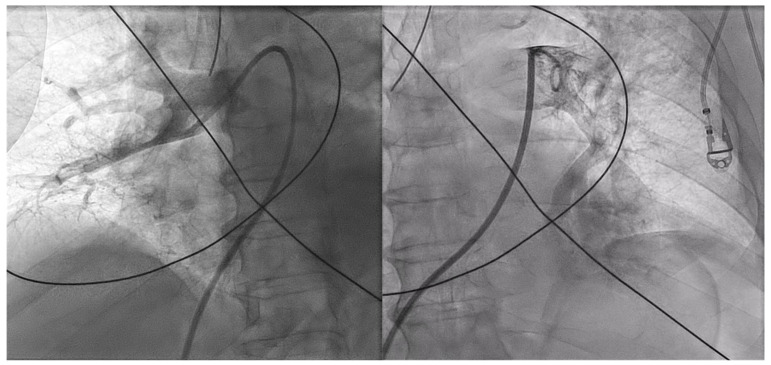
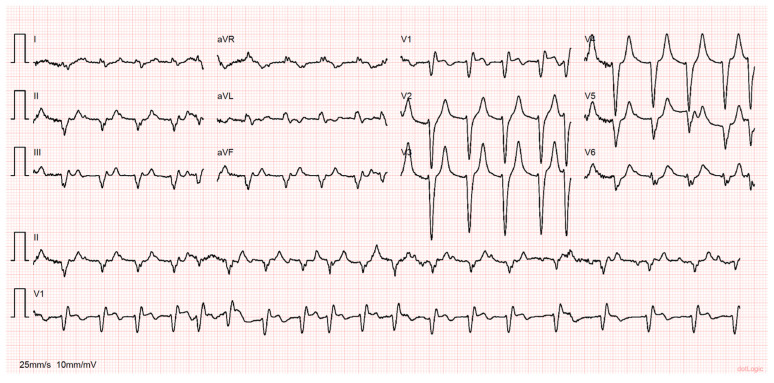
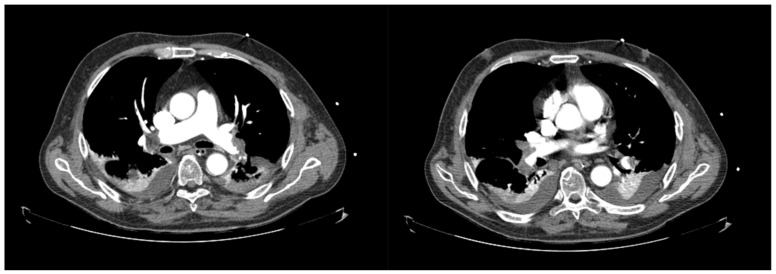
The clinical presentation of pulmonary embolism (PE) and acute coronary syndrome can be similar. We report a case of a patient presenting with antero-septal ST-segment elevation after cardiac arrest, found to have acute-PE-mimicking ST-segment elevation myocardial infarction (STEMI), treated with aspiration thrombectomy and catheter-directed thrombolysis (CDT). A 78-year-old man was admitted with dyspnea, chest pain and tachycardia. During evaluation, cardiac arrest in pulseless electrical activity was documented. Advanced life support was started immediately. ECG post-ROSC revealed ST-segment elevation in V1-V4 and aVR. Echocardiography showed normal left ventricular function but right ventricular (RV) dilation and severe dysfunction. The patient was in shock and was promptly referred to cardiac catheterization that excluded significant CAD. Due to the discordant ECG and echocardiogram findings, acute PE was suspected, and immediate invasive pulmonary angiography revealed bilateral massive pulmonary embolism. Successful aspiration thrombectomy was performed followed by local alteplase infusion. At the end of the procedure, mPAP was reduced and blood pressure normalized allowing withdrawal of vasopressor support. Twenty-four-hour echocardiographic reassessment showed normal-sized cardiac chambers with preserved biventricular systolic function. Bedside echocardiography in patients with ST-segment elevation post-ROSC is instrumental in raising the suspicion of acute PE. In the absence of a culprit coronary lesion, prompt pulmonary angiography should be considered if immediately feasible. In these cases, CDT and aspiration in high-risk acute PE seem safe and effective in relieving obstructive shock and restoring hemodynamics.
肺栓塞(PE)和急性冠状动脉综合征的临床表现可能相似。我们报告一例患者,心脏骤停后出现前间隔ST段抬高,经检查发现为急性PE模拟ST段抬高型心肌梗死(STEMI),接受了抽吸血栓切除术和导管定向溶栓(CDT)治疗。一名78岁男性因呼吸困难、胸痛和心动过速入院。评估期间,记录到无脉电活动导致的心脏骤停。立即启动了高级生命支持。恢复自主循环(ROSC)后的心电图显示V1-V4和aVR导联ST段抬高。超声心动图显示左心室功能正常,但右心室(RV)扩张且严重功能障碍。患者处于休克状态,迅速被转诊至心脏导管检查,排除了严重冠状动脉疾病(CAD)。由于心电图和超声心动图结果不一致,怀疑为急性PE,立即进行的有创肺血管造影显示双侧大面积肺栓塞。成功实施了抽吸血栓切除术,随后局部注入阿替普酶。手术结束时,平均肺动脉压(mPAP)降低,血压恢复正常,可停用血管升压药支持。24小时超声心动图复查显示心脏腔室大小正常,双心室收缩功能保留。ROSC后出现ST段抬高的患者床边超声心动图有助于提高对急性PE的怀疑。在没有罪犯冠状动脉病变的情况下,如果立即可行,应考虑及时进行肺血管造影。在这些病例中,CDT和高危急性PE的抽吸在缓解梗阻性休克和恢复血流动力学方面似乎是安全有效的。