Liu Christina, Zhang Dafang, Blazar Philip, Earp Brandon E
Division of Hand and Upper-Extremity Surgery, Department of Orthopedics, Brigham and Women's Hospital, Boston.
Harvard Medical School, Boston, MA.
J Hand Surg Glob Online. 2023 Jun 4;5(5):612-619. doi: 10.1016/j.jhsg.2023.05.006. eCollection 2023 Sep.
Compare outcomes of acute versus delayed total elbow arthroplasty (TEA) following distal humerus fractures (DHF).
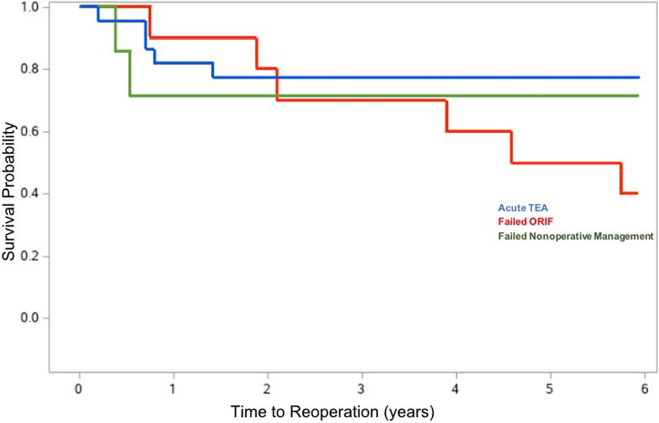
This retrospective study included 39 patients who underwent primary TEA with semiconstrained implants for DHF, either within 4 weeks of their injury or after failing initial open reduction and internal fixation (ORIF) or nonsurgical management, between June 1, 2003 and February 1, 2018 with minimum 1-year follow-up. Our outcome measures included DASH (Disabilities of the Arm, Shoulder, and Hand) score, complications, reoperations, and range of motion (ROM). Demographics, clinical variables, and outcomes were compared using the Student's -test, Mann-Whitney U test, and Fisher's exact test as appropriate. Kaplan-Meier curves for mortality, implant survivorship, and reoperation were created.
Our patients were categorized into acute TEA (n = 22), ORIF to TEA (n = 10), and nonsurgical to TEA (n = 7) treatment groups. Additional analysis was performed comparing acute to delayed TEA, which combined data from failed ORIF and nonsurgical cohorts. The median follow-up, average age, and median Charlson comorbility index were similar between groups. The most common fracture pattern was AO13C. At median follow-up of 5.8 years, DASH differed between cohorts: mean of 31 (SD 19) in acute TEA and 52 (SD 27) in delayed TEA, which further subdivided to 44.2 (SD 25) in failed ORIF and 76 (SD 23) in failed nonsurgical management. Poorer DASH scores at final follow-up were associated with delayed TEA, initial nonsurgical management, and depression. Surgical complications were associated with delayed TEA. Higher Charlson comorbidity index was associated with death. No variables were associated significantly with ROM, revision, or reoperation.
Comminuted DHFs are difficult to treat in the elderly with high rates of complication and poor function after surgery. Our study suggests TEA performed acutely result in satisfactory outcomes and should be a consideration for patients at high risk of failing ORIF or nonsurgical management.
TYPE OF STUDY/LEVEL OF EVIDENCE: Therapeutic, III.
比较肱骨远端骨折(DHF)后急性与延迟全肘关节置换术(TEA)的疗效。
这项回顾性研究纳入了39例因DHF接受半限制型假体初次TEA的患者,这些患者在2003年6月1日至2018年2月1日期间受伤后4周内,或在初次切开复位内固定(ORIF)或非手术治疗失败后接受手术,且至少随访1年。我们的疗效指标包括上肢、肩部和手部功能障碍(DASH)评分、并发症、再次手术以及活动范围(ROM)。根据情况,使用学生t检验、曼-惠特尼U检验和费舍尔精确检验对人口统计学、临床变量和疗效进行比较。绘制了死亡率、假体生存率和再次手术的Kaplan-Meier曲线。
我们的患者被分为急性TEA治疗组(n = 22)、ORIF转为TEA治疗组(n = 10)和非手术转为TEA治疗组(n = 7)。对急性与延迟TEA进行了额外分析,将ORIF失败和非手术队列的数据合并。各组之间的中位随访时间、平均年龄和中位查尔森合并症指数相似。最常见的骨折类型是AO13C。在中位随访5.8年时,各队列之间的DASH评分有所不同:急性TEA组的平均评分为31(标准差19),延迟TEA组为52(标准差27),其中ORIF失败组进一步细分为44.2(标准差25),非手术治疗失败组为76(标准差23)。最终随访时较差的DASH评分与延迟TEA、初始非手术治疗和抑郁有关。手术并发症与延迟TEA有关。较高的查尔森合并症指数与死亡有关。没有变量与ROM、翻修或再次手术有显著关联。
粉碎性DHF在老年人中难以治疗,术后并发症发生率高且功能差。我们的研究表明,急性进行TEA可取得满意的疗效,对于有ORIF或非手术治疗失败高风险的患者应予以考虑。
研究类型/证据水平:治疗性研究,III级。