Feinstein Shawn D, Paterno Anthony V, Allen Andrew D, Jewell Emily, Wright Sarah T, Draeger Reid W
Department of Orthopaedics, University of North Carolina, Chapel Hill, NC.
University Libraries, University of North Carolina, Chapel Hill, NC.
J Hand Surg Glob Online. 2023 Jun 16;5(5):643-649. doi: 10.1016/j.jhsg.2023.04.001. eCollection 2023 Sep.
We aimed to characterize the incidence of complications regarding olecranon osteotomy, looking more specifically at the type of osteotomy and the fixation construct used to repair the osteotomy.
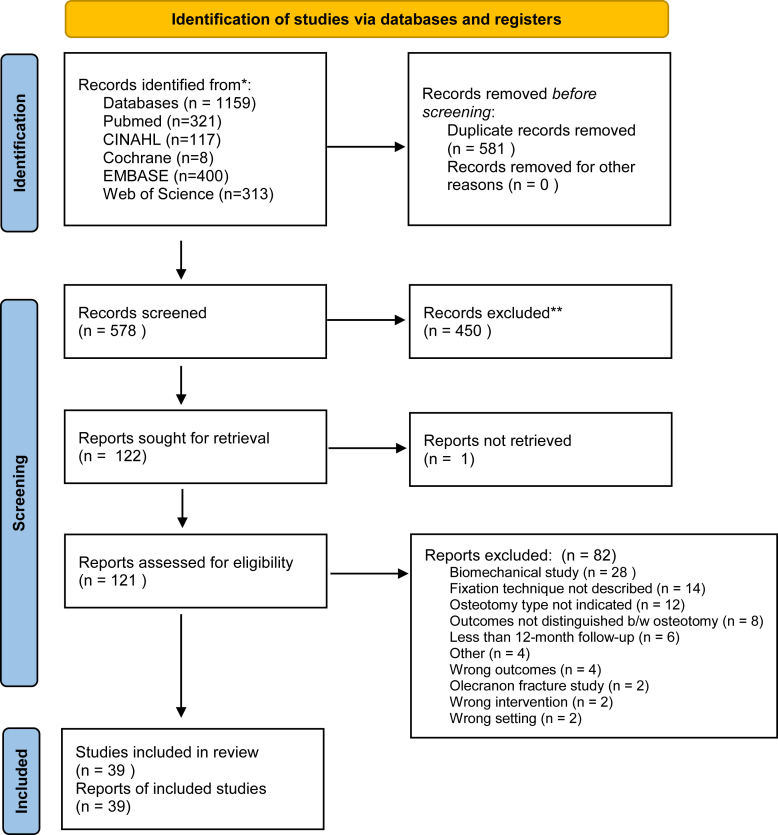
In accordance with Preferred Reporting Items for Systematic Reviews and Meta-Analyses guidelines, a comprehensive search was performed. A study was included if it was an adult clinical study, a transverse or chevron olecranon osteotomy was performed, and the study explicitly states the fixation construct used to repair the osteotomy. A quality assessment was performed in each study prior to data extraction.
We included 39 studies with a total of 1,445 patients. Most studies included patients who were being treated primarily for a distal humerus fracture. The overall incidence of delayed union was 27/643 (4.2%), with a higher rate in transverse osteotomy than in chevron osteotomy (5/49 (10.2%) vs 22/595 (3.7%)). Nonunion occurred in 43/811 (5.4%) of patients, with a higher rate in transverse osteotomy (6/73 (8.2%) vs. 37/712 (5.2%)). Implant failure or loss of reduction occurred in 44/746 (5.9%) of patients, with a higher rate in transverse osteotomy (11/49 (22.4%) vs 33/688 (4.8%)). The removal of implants occurred in 236/1078 (21.9%) of all patients, with the highest rate in those studies that used plate fixation 44/99 (44.4%).
Compared with chevron osteotomy, patients who underwent transverse osteotomy had a higher incidence of delayed union, nonunion, and implant failure or loss of reduction requiring revision surgery. The incidence of implant removal indicates that patients should be informed that nearly half of the osteotomy fixed with a plate was removed after implantation.
TYPE OF STUDY/LEVEL OF EVIDENCE: Therapeutic III.
我们旨在描述尺骨鹰嘴截骨术并发症的发生率,更具体地关注截骨术的类型以及用于修复截骨术的固定结构。
按照系统评价和Meta分析的首选报告项目指南进行全面检索。纳入的研究需为成人临床研究,进行了横形或V形尺骨鹰嘴截骨术,且研究明确说明了用于修复截骨术的固定结构。在数据提取前对每项研究进行质量评估。
我们纳入了39项研究,共1445例患者。大多数研究纳入的患者主要因肱骨远端骨折接受治疗。延迟愈合的总体发生率为27/643(4.2%),横形截骨术的发生率高于V形截骨术(5/49(10.2%)对22/595(3.7%))。骨不连发生在43/811(5.4%)的患者中,横形截骨术的发生率更高(6/73(8.2%)对37/712(5.2%))。内植物失败或复位丢失发生在44/746(5.9%)的患者中,横形截骨术的发生率更高(11/49(22.4%)对33/688(4.8%))。所有患者中有236/1078(21.9%)进行了内植物取出,在使用钢板固定的研究中发生率最高,为44/99(44.4%)。
与V形截骨术相比,接受横形截骨术的患者延迟愈合、骨不连以及内植物失败或复位丢失需要翻修手术的发生率更高。内植物取出的发生率表明,应告知患者,用钢板固定的截骨术中近一半在植入后被取出。
研究类型/证据水平:治疗性III级。