Ocak Ilhan
Department of Liver Transplant Critical Care Medicine, Memorial Sisli Hospital, Istanbul, Türkiye.
Front Med (Lausanne). 2023 Sep 22;10:1190067. doi: 10.3389/fmed.2023.1190067. eCollection 2023.
Acute liver failure (ALF) is a serious condition characterized by sudden liver dysfunction, jaundice and hepatic encephalopathy. Its mortality rate of approximately 80% underscores the urgent need for effective treatments. Supportive extracorporeal therapies (SET), which temporarily support liver function and remove toxins, have shown promise in improving outcomes in acute liver failure (ALF). The aim of this study was to compare the outcomes of dual supportive extracorporeal therapy (SET) and mono supportive extracorporeal therapy in patients with acute liver failure.
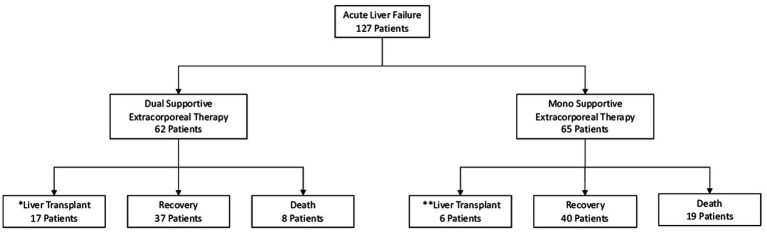
A total of 127 patients with acute liver failure were included in this retrospective, single-center study. Of these, 62 patients received dual supportive extracorporeal therapy and 65 patients received mono supportive extracorporeal therapy. Primary endpoints were survival without the need for liver transplantation and mortality. Secondary endpoints included resolution of encephalopathy and normalization of International Normalized Ratio (INR).
In the dual supportive extracorporeal therapy group, 59.6% of patients survived without the need for liver transplantation, while 27.4% achieved recovery with liver transplantation. The mortality rate in this group was 12.9%. Significant regression of encephalopathy grade was observed in 87% of patients, and the 1 year mortality rate for liver transplant recipients was 10.7%. In the mono supportive extracorporeal therapy group, 61.5% of patients experienced a successful recovery without the need for liver transplantation, with a mortality rate of 29.2%. Significant improvement in the grade of encephalopathy was observed in 70.7% of patients.
Both dual supportive extracorporeal therapy (CVVHDF and PE) and mono supportive extracorporeal therapy (PE) were associated with significant improvements in renal and hepatic biochemical parameters, blood ammonia levels, and neurological status in patients with acute liver failure associated with grade III-IV hepatic encephalopathy. In particular, dual support was associated with improved hemodynamic stability, lactic acidosis and acid-base balance. Survival in acute liver failure in our retrospective cohort using a protocolized approach to extracorporeal therapies is higher compared to previously published large ALF studies. This protocolized approach warrants further prospective studies.
急性肝衰竭(ALF)是一种严重疾病,其特征为肝功能突然受损、黄疸和肝性脑病。其约80%的死亡率凸显了对有效治疗的迫切需求。支持性体外治疗(SET)可暂时支持肝功能并清除毒素,已显示出改善急性肝衰竭(ALF)患者预后的前景。本研究旨在比较双重支持性体外治疗(SET)和单一支持性体外治疗对急性肝衰竭患者的疗效。
本项回顾性单中心研究共纳入127例急性肝衰竭患者。其中,62例患者接受双重支持性体外治疗,65例患者接受单一支持性体外治疗。主要终点为无需肝移植的生存率和死亡率。次要终点包括脑病的缓解以及国际标准化比值(INR)的正常化。
在双重支持性体外治疗组中,59.6%的患者无需肝移植而存活,27.4%的患者通过肝移植实现康复。该组死亡率为12.9%。87%的患者脑病分级显著改善,肝移植受者的1年死亡率为10.7%。在单一支持性体外治疗组中,61.5%的患者无需肝移植而成功康复,死亡率为29.2%。70.7%的患者脑病分级有显著改善。
双重支持性体外治疗(连续性静脉-静脉血液透析滤过和血浆置换)和单一支持性体外治疗(血浆置换)均与III-IV级肝性脑病相关的急性肝衰竭患者的肾脏和肝脏生化参数、血氨水平及神经状态的显著改善有关。特别是,双重支持与改善血流动力学稳定性、乳酸性酸中毒及酸碱平衡有关。与先前发表的大型急性肝衰竭研究相比,我们采用体外治疗方案的回顾性队列中急性肝衰竭患者的生存率更高。这种方案化方法值得进一步开展前瞻性研究。