Department of Ophthalmology, Faculty of Medicine, University of Alexandria, Postal Code 21523, 19 Amin Fekry Street, Raml Station, Alexandria, Egypt.
Department of Ophthalmology, University of Ngozi, Ngozi, Burundi.
Int Ophthalmol. 2023 Dec;43(12):4837-4849. doi: 10.1007/s10792-023-02886-w. Epub 2023 Oct 20.
The purpose of this prospective study was to evaluate the effect of combined photorefractive keratectomy (PRK) and corneal collagen cross-linking (CXL) on intraocular pressure (IOP) in patients with keratoconus (KC).
We included 64 eyes of 34 patients (19 males and 15 females; age: 19-40y) with stages 1-2 keratoconus which had undergone combined wavefront-optimized photorefractive keratectomy and corneal collagen cross linking. Two other groups of patients were added as controls: the PRK group including 110 eyes of 57 patients (23 males and 34 females; age: 18-44y) which had undergone wavefront-optimized photorefractive keratectomy for myopic refractive errors, and the CXL group including 36 eyes of 23 patients (14 males and 9 females; age: 12-38y) with keratoconus, not filling the inclusion criteria for combined PRK and CXL, which had undergone corneal collagen cross-linking. IOP was recorded preoperatively and postoperatively at 3, 6 and 12 months follow-up visits.
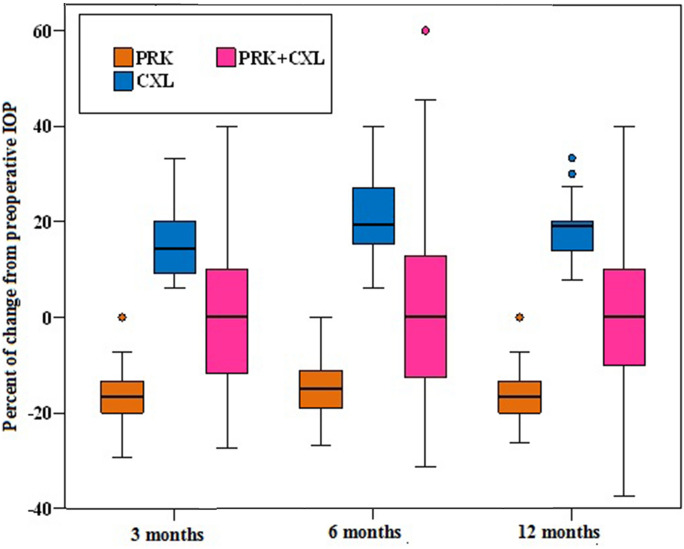
Preoperative IOP in both CXL (12.1 ± 2.53 mmHg) and PRK + CXL (13.2 ± 2.50 mmHg) groups was significantly lower than PRK group (15.8 ± 3.10 mmHg) (F = 30.505, p < 0.001). At 3 months postoperatively, IOP showed no statistically significant difference between the three studied groups (F = 1.821, p = 0.164). At 6 months postoperatively, IOP in the CXL group (14.6 ± 2.64 mmHg) was significantly higher than both PRK (13.4 ± 2.27 mmHg) and PRK + CXL (13.3 ± 2.62 mmHg) groups (F = 3.721, p = 0.026). At 12 months postoperatively, IOP in the CXL group (14.3 ± 2.69 mmHg) was significantly higher than the PRK group (13.2 ± 2.23 mmHg) and was higher than PRK + CXL group (13.3 ± 2.59 mmHg) although not statistically significant (F = 3.393, p = 0.035). Regarding the percent of change from preoperative IOP, a statistically significant difference between the three studied groups was detected at 3, 6 and 12 months postoperatively (H = 117.459, 109.303, 122.694 respectively, p < 0.001). The median percent of change from preoperative IOP in the PRK group was -16.7%, -15%, and -16.7%, in the CXL group was + 14.3%, + 19.4%, and + 19.1%, while in PRK + CXL group was 0% at 3, 6 and 12 months postoperatively. (Post-hoc power analysis 75%).
Combined PRK and CXL in patients with KC shows no significant effect on IOP, in contrast to either procedure performed separately.
本前瞻性研究旨在评估角膜胶原交联术(CXL)联合准分子激光角膜表面切削术(PRK)治疗圆锥角膜(KC)患者眼压(IOP)的效果。
纳入 34 例(19 名男性和 15 名女性;年龄:19-40 岁)1-2 级圆锥角膜患者,均接受波前引导优化的 PRK 联合角膜胶原交联术。另外加入两组对照患者:接受波前引导优化的 PRK 治疗近视屈光不正的 PRK 组,共 110 只眼(23 名男性和 34 名女性;年龄:18-44 岁);角膜胶原交联术组,共 36 只眼(14 名男性和 9 名女性;年龄:12-38 岁),角膜胶原交联术不符合联合 PRK 和 CXL 的纳入标准,共 23 例患者。记录术前及术后 3、6 和 12 个月的眼压。
CXL(12.1±2.53mmHg)和 PRK+CXL(13.2±2.50mmHg)组的术前 IOP 明显低于 PRK 组(15.8±3.10mmHg)(F=30.505,p<0.001)。术后 3 个月,三组间 IOP 无统计学差异(F=1.821,p=0.164)。术后 6 个月,CXL 组 IOP(14.6±2.64mmHg)明显高于 PRK 组(13.4±2.27mmHg)和 PRK+CXL 组(13.3±2.62mmHg)(F=3.721,p=0.026)。术后 12 个月,CXL 组 IOP(14.3±2.69mmHg)高于 PRK 组(13.2±2.23mmHg),但与 PRK+CXL 组(13.3±2.59mmHg)无统计学差异(F=3.393,p=0.035)。关于从术前 IOP 的百分比变化,术后 3、6 和 12 个月三组间差异有统计学意义(H=117.459、109.303、122.694,p<0.001)。PRK 组术后 3、6 和 12 个月的术前 IOP 百分比变化中位数分别为-16.7%、-15%和-16.7%,CXL 组分别为+14.3%、+19.4%和+19.1%,PRK+CXL 组分别为 0%。(后验功效分析 75%)。
与单独进行的手术相比,KC 患者的 PRK 和 CXL 联合治疗对 IOP 无显著影响。