De Geyter C, Matt L, De Geyter I, Moffat R, Meier C
Reproductive Medicine and Gynecological Endocrinology (RME), University Hospital, University of Basel, Basel, Switzerland.
Division of Endocrinology, Diabetes & Metabolism, University Hospital Basel, University of Basel, Basel, Switzerland.
Hum Reprod Open. 2023 Oct 9;2023(4):hoad038. doi: 10.1093/hropen/hoad038. eCollection 2023.
How does subclinical hypothyroidism, defined in infertile women during preconception by thyroid-stimulating hormone (TSH) >2.5 or >4.5 mIU/l, with or without thyroid peroxidase antibodies (anti-TPO) >100 IU/ml, impact thyroid hormone levels during pregnancy and after birth?
During pregnancy, TSH levels remain similar to those in preconception, even with supplementary thyroxine, whereas the serum levels of anti-TPO progressively decline.
Overt hypothyroidism impacts both pregnancy and offspring but randomized clinical trials and cohort studies failed to detect the benefit of treatment with thyroxine in cases with low-threshold TSH or with anti-TPO during pregnancy.
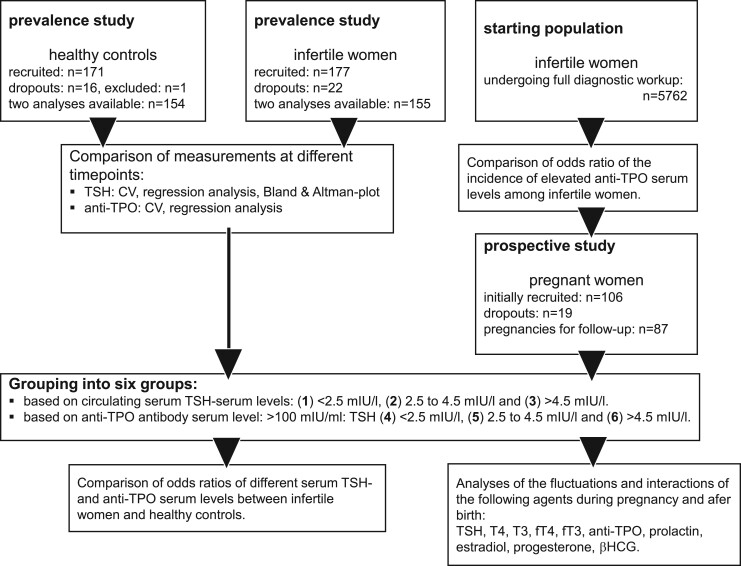
First, the prevalence and reproducibility of two candidate cut-off levels of subclinical hypothyroidism in a cohort of 177 infertile women was compared with 171 women not aiming for pregnancy. Second, the impact of distinct setpoints of TSH in preconception (with or without anti-TPO) was monitored during pregnancy in 87 previously infertile women by high-frequency monitoring of thyroid function. Both studies were carried out from 2007 to 2019.
PARTICIPANTS/MATERIALS SETTING METHODS: Reproducibility and prevalence of subclinical hypothyroidism were examined in infertile women presenting in the fertility care unit of an academic institution. Women not aiming for pregnancy participated as controls. In both groups, TSH and anti-TPO were measured two times on different occasions. In addition, a group of previously infertile women with known preconception setpoints of TSH (with or without anti-TPO) were followed up prospectively throughout pregnancy and after birth. During pregnancy, serum was sampled weekly until Week 12, then monthly until delivery, and once after birth. Only cases with preconception TSH >4.5 mIU/l were supplemented with thyroxine. After collection of all samples, the serum levels of anti-TPO and the major thyroid hormones were measured. Prolactin with known fluctuations during pregnancy was used as reference.
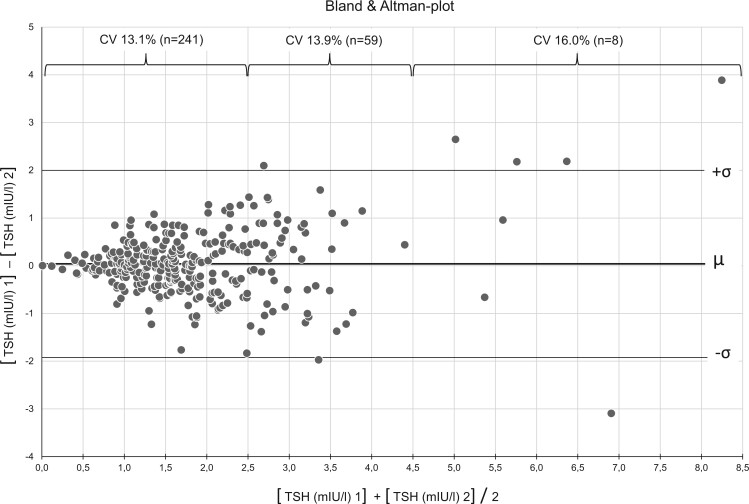
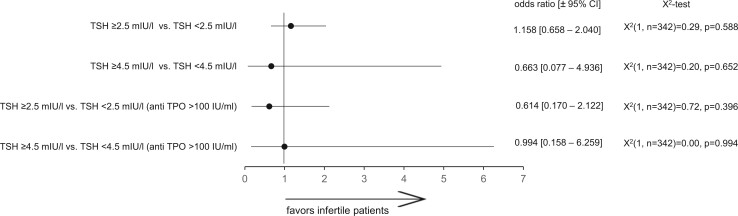
Measures of both TSH and anti-TPO at two different time points were accurate and reproducible. The odds of subclinical hypothyroidism in infertile women and controls were similar. During pregnancy, TSH closely followed preconception TSH levels, whereas serum levels of the thyroid hormones predominantly remained within or above (not below) the reference. Treatment of infertile women with preconception TSH >4.5 mIU/l with thyroxine resulted in higher free thyroxine (fT4) serum levels. The serum levels of anti-TPO declined as pregnancies evolved.
The numbers of participants both in the prevalence study and in pregnancy did not reach the estimated numbers. For ethical reasons, the patients with preconception TSH >4.5 mIU/l were treated with thyroxine. The findings apply to infertile women only.
We propose to use >4.5 mIU/l as the serum TSH threshold for supplementing women with thyroxine before pregnancy. During pregnancy, fT4 may be the better marker to monitor thyroid function. The consistent decrease of anti-TPO antibody levels during ongoing pregnancies must be considered a protective element.
STUDY FUNDING/COMPETING INTERESTS: The prevalence part of this study was supported by Merck-Serono, Geneva (TH006/EMR200007-603). The hormone measurements of the serum samples collected during the follow-up pregnancies were made possible by financial support of Roche Diagnostica (November 1721, 2017, Rotkreuz, Switzerland). I.D.G. was supported by a grant of the Repronatal Foundation, Basel, Switzerland. All authors declare no conflict of interest.
Research Database of UniBasel, project no. 576691 (2007).
在孕前通过促甲状腺激素(TSH)>2.5或>4.5 mIU/l定义的亚临床甲状腺功能减退,无论有无甲状腺过氧化物酶抗体(抗-TPO)>100 IU/ml,对孕期及产后甲状腺激素水平有何影响?
孕期TSH水平即使补充甲状腺素仍与孕前相似,而抗-TPO血清水平逐渐下降。
显性甲状腺功能减退对妊娠和后代均有影响,但随机临床试验和队列研究未能检测出孕期低阈值TSH或抗-TPO患者接受甲状腺素治疗的益处。
研究设计、规模、持续时间:首先,比较了177名不孕女性队列中两个亚临床甲状腺功能减退候选切点水平的患病率和可重复性,并与171名未计划怀孕的女性进行对比。其次,通过高频监测甲状腺功能,对87名既往不孕女性孕前不同TSH设定点(有无抗-TPO)在孕期的影响进行监测。两项研究均在2007年至2019年开展。
参与者/材料、设置、方法:在一所学术机构的生殖保健科就诊的不孕女性中检测亚临床甲状腺功能减退的可重复性和患病率。未计划怀孕的女性作为对照。两组均在不同时间测量两次TSH和抗-TPO。此外,对一组已知孕前TSH设定点(有无抗-TPO)的既往不孕女性在孕期及产后进行前瞻性随访。孕期每周采血直至第12周,之后每月采血直至分娩,产后采血一次。仅孕前TSH>4.5 mIU/l的患者补充甲状腺素。收集所有样本后,检测抗-TPO和主要甲状腺激素的血清水平。将孕期波动已知的催乳素用作对照。
两个不同时间点的TSH和抗-TPO测量准确且可重复。不孕女性和对照中亚临床甲状腺功能减退的几率相似。孕期TSH紧密跟随孕前TSH水平,而甲状腺激素血清水平主要保持在参考值范围内或之上(而非之下)。孕前TSH>4.5 mIU/l的不孕女性接受甲状腺素治疗后,血清游离甲状腺素(fT4)水平升高。随着孕期进展,抗-TPO血清水平下降。
局限性、谨慎理由:患病率研究和孕期研究的参与者数量均未达到预期数量。出于伦理原因,孕前TSH>4.5 mIU/l的患者接受了甲状腺素治疗。研究结果仅适用于不孕女性。
我们建议将>4.5 mIU/l作为孕前女性补充甲状腺素的血清TSH阈值。孕期,fT4可能是监测甲状腺功能的更好指标。孕期抗-TPO抗体水平持续下降必须被视为一种保护因素。
研究资金/利益冲突:本研究的患病率部分由日内瓦的默克雪兰诺公司(TH006/EMR200007 - 603)资助。后续孕期收集的血清样本的激素检测由罗氏诊断公司(2017年11月17日至21日,瑞士罗特kreuz)提供资金支持得以实现。I.D.G.得到了瑞士巴塞尔生殖医学基金会的资助。所有作者均声明无利益冲突。
巴塞尔大学研究数据库,项目编号576691(2007年)