Quantitative Sciences Unit, Stanford University School of Medicine, Stanford, California.
Department of Neurosurgery, Stanford University School of Medicine, Stanford, California.
JAMA Oncol. 2023 Dec 1;9(12):1640-1648. doi: 10.1001/jamaoncol.2023.4447.
The revised 2021 US Preventive Services Task Force (USPSTF) guidelines for lung cancer screening have been shown to reduce disparities in screening eligibility and performance between African American and White individuals vs the 2013 guidelines. However, potential disparities across other racial and ethnic groups in the US remain unknown. Risk model-based screening may reduce racial and ethnic disparities and improve screening performance, but neither validation of key risk prediction models nor their screening performance has been examined by race and ethnicity.
To validate and recalibrate the Prostate, Lung, Colorectal, and Ovarian Cancer Screening Trial 2012 (PLCOm2012) model-a well-established risk prediction model based on a predominantly White population-across races and ethnicities in the US and evaluate racial and ethnic disparities and screening performance through risk-based screening using PLCOm2012 vs the USPSTF 2021 criteria.
DESIGN, SETTING, AND PARTICIPANTS: In a population-based cohort design, the Multiethnic Cohort Study enrolled participants in 1993-1996, followed up through December 31, 2018. Data analysis was conducted from April 1, 2022, to May 19. 2023. A total of 105 261 adults with a smoking history were included.
The 6-year lung cancer risk was calculated through recalibrated PLCOm2012 (ie, PLCOm2012-Update) and screening eligibility based on a 6-year risk threshold greater than or equal to 1.3%, yielding similar eligibility as the USPSTF 2021 guidelines.
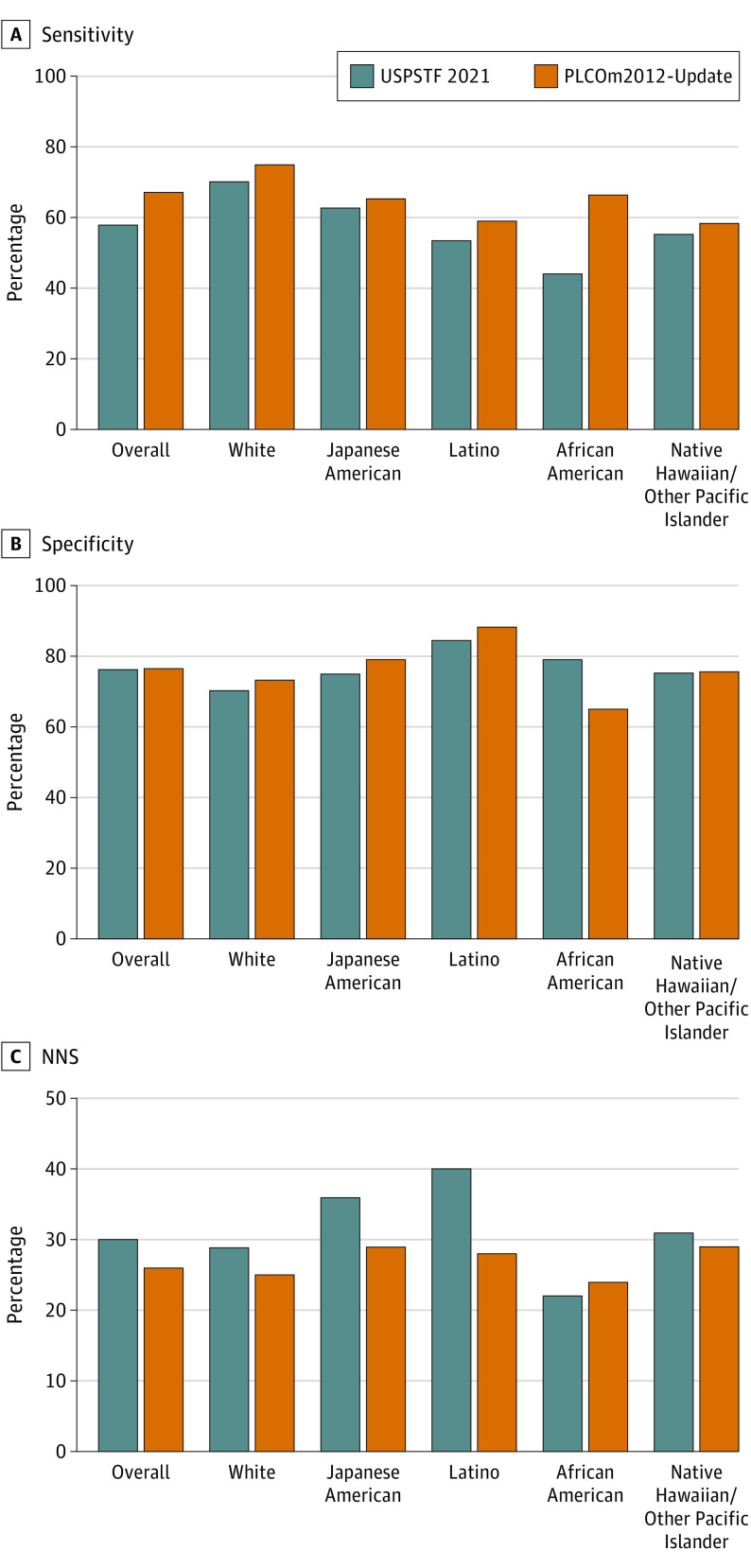
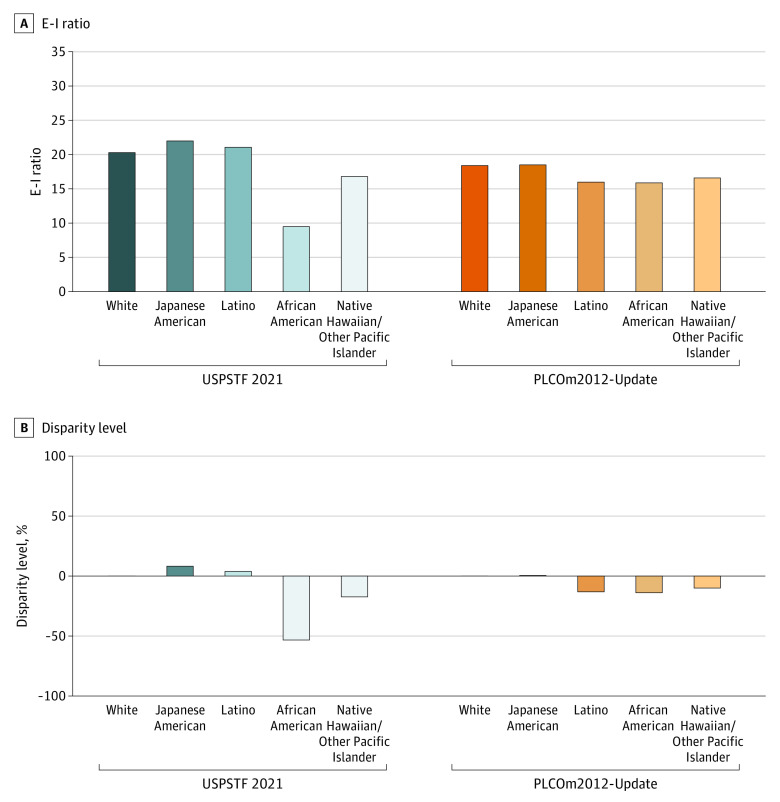
Predictive accuracy, screening eligibility-incidence (E-I) ratio (ie, ratio of the number of eligible to incident cases), and screening performance (sensitivity, specificity, and number needed to screen to detect 1 lung cancer).
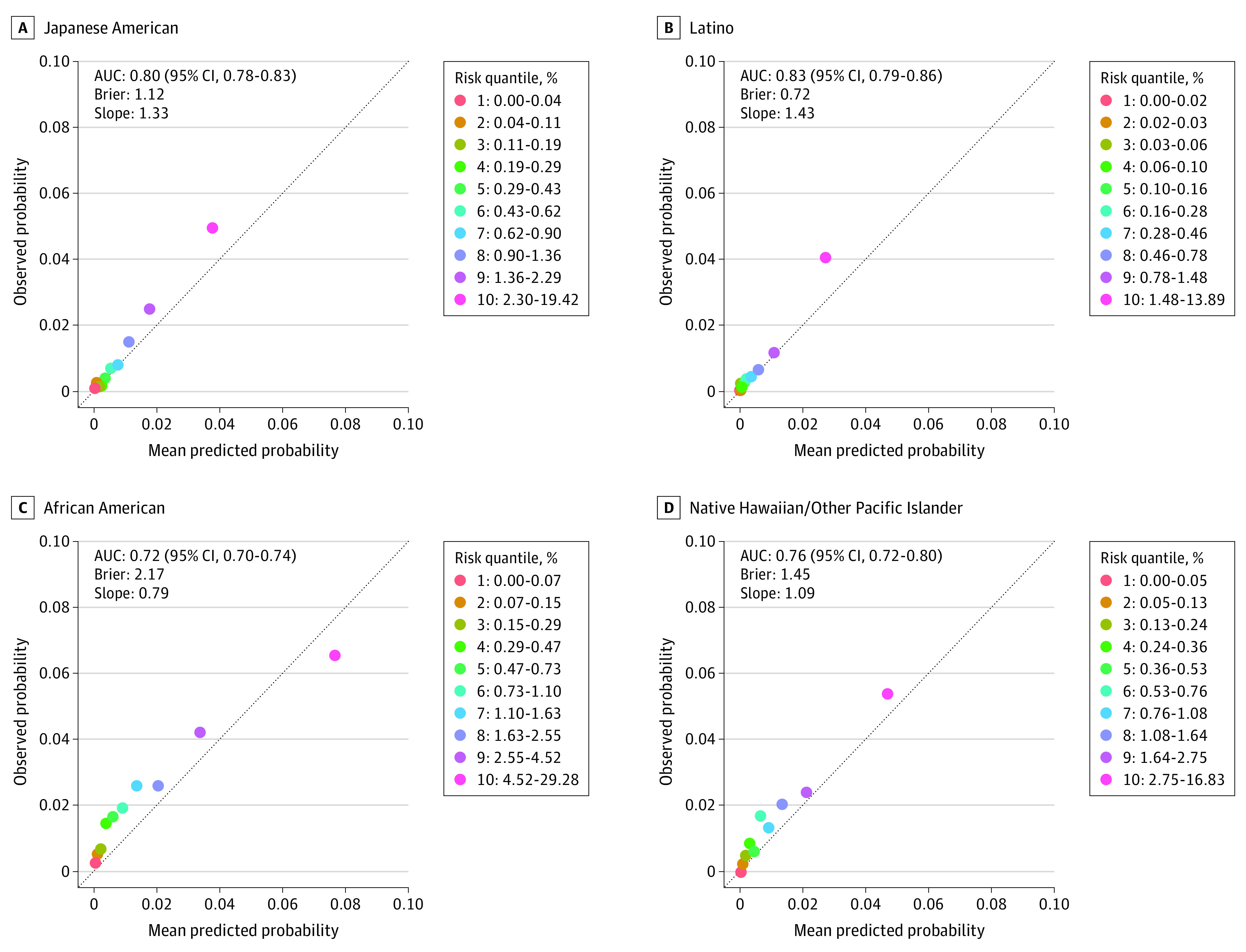
Of 105 261 participants (60 011 [57.0%] men; mean [SD] age, 59.8 [8.7] years), consisting of 19 258 (18.3%) African American, 27 227 (25.9%) Japanese American, 21 383 (20.3%) Latino, 8368 (7.9%) Native Hawaiian/Other Pacific Islander, and 29 025 (27.6%) White individuals, 1464 (1.4%) developed lung cancer within 6 years from enrollment. The PLCOm2012-Update showed good predictive accuracy across races and ethnicities (area under the curve, 0.72-0.82). The USPSTF 2021 criteria yielded a large disparity among African American individuals, whose E-I ratio was 53% lower vs White individuals (E-I ratio: 9.5 vs 20.3; P < .001). Under the risk-based screening (PLCOm2012-Update 6-year risk ≥1.3%), the disparity between African American and White individuals was substantially reduced (E-I ratio: 15.9 vs 18.4; P < .001), with minimal disparities observed in persons of other minoritized groups, including Japanese American, Latino, and Native Hawaiian/Other Pacific Islander. Risk-based screening yielded superior overall and race and ethnicity-specific performance to the USPSTF 2021 criteria, with higher overall sensitivity (67.2% vs 57.7%) and lower number needed to screen (26 vs 30) at similar specificity (76.6%).
The findings of this cohort study suggest that risk-based lung cancer screening can reduce racial and ethnic disparities and improve screening performance across races and ethnicities vs the USPSTF 2021 criteria.
修订后的 2021 年美国预防服务工作组(USPSTF)肺癌筛查指南已被证明可以减少非裔美国人和白种人之间在筛查资格和表现方面的差异,而不是 2013 年的指南。然而,在美国,其他种族和族裔群体的潜在差异仍不得而知。基于风险模型的筛查可能会减少种族和族裔差异,并提高筛查性能,但关键风险预测模型的验证及其筛查性能都没有按种族和族裔进行检查。
验证和重新校准前列腺癌、肺癌、结直肠癌和卵巢癌筛查试验 2012 年(PLCOm2012)模型——这是一个基于主要是白人人口的成熟风险预测模型——在美国的各种种族和族裔中,并通过基于风险的筛查使用 PLCOm2012 与 USPSTF 2021 标准来评估种族和族裔差异和筛查性能。
设计、地点和参与者:在基于人群的队列设计中,多民族队列研究于 1993 年至 1996 年招募参与者,并在 2018 年 12 月 31 日之前进行随访。数据分析于 2022 年 4 月 1 日至 2023 年 5 月 19 日进行。共有 105261 名有吸烟史的成年人被纳入。
通过重新校准的 PLCOm2012(即 PLCOm2012-Update)计算 6 年肺癌风险,并根据 6 年风险大于或等于 1.3%的标准计算筛查资格,从而产生与 USPSTF 2021 指南相似的资格。
在 105261 名参与者中(60011 名[57.0%]为男性;平均[标准差]年龄为 59.8[8.7]岁),包括 19258 名(18.3%)非裔美国人、27227 名(25.9%)日裔美国人、21383 名(20.3%)拉丁裔、8368 名(7.9%)美国原住民/其他太平洋岛民和 29025 名(27.6%)白人,1464 名(1.4%)在入组后 6 年内发生肺癌。PLCOm2012-Update 在各种种族和族裔中表现出良好的预测准确性(曲线下面积,0.72-0.82)。USPSTF 2021 标准在非裔美国人中产生了很大的差异,其 E-I 比率比白人低 53%(E-I 比率:9.5 与 20.3;P<0.001)。在基于风险的筛查(PLCOm2012-Update 6 年风险≥1.3%)下,非裔美国人和白人之间的差异大大减少(E-I 比率:15.9 与 18.4;P<0.001),包括日裔美国人、拉丁裔和美国原住民/其他太平洋岛民在内的其他少数族裔的差异极小。基于风险的筛查在整体和种族和族裔特异性性能方面优于 USPSTF 2021 标准,具有更高的总体敏感性(67.2%比 57.7%)和更低的需要筛查的人数(26 与 30),特异性相似(76.6%)。
这项队列研究的结果表明,基于风险的肺癌筛查可以减少种族和族裔差异,并提高与 USPSTF 2021 标准相比的筛查性能。