Rolling Julie, Rabot Juliette, Reynaud Eve, Kolb Oriane, Bourgin Patrice, Schroder Carmen M
Department of Child and Adolescent Psychiatry, Strasbourg University Hospital, 67091 Strasbourg, France.
Regional Center for Psychotraumatism Great East, Strasbourg University Hospital, 67091 Strasbourg, France.
J Clin Med. 2023 Oct 17;12(20):6570. doi: 10.3390/jcm12206570.
Sleep disturbances (insomnia and nightmare symptoms) are the most sensitive and persistent symptoms of pediatric post-traumatic stress disorder (PTSD). Untreated, these sleep disturbances (SD) associated with PTSD are predictive of PTSD persistence and increased psychiatric complications. The aim of this study was to evaluate sleep and circadian rhythms in children with PTSD under both laboratory and ecological conditions in comparison with a control population and to test for the first time the hypothesis that SD and circadian rhythms are positively correlated with PTSD severity and its comorbidities.
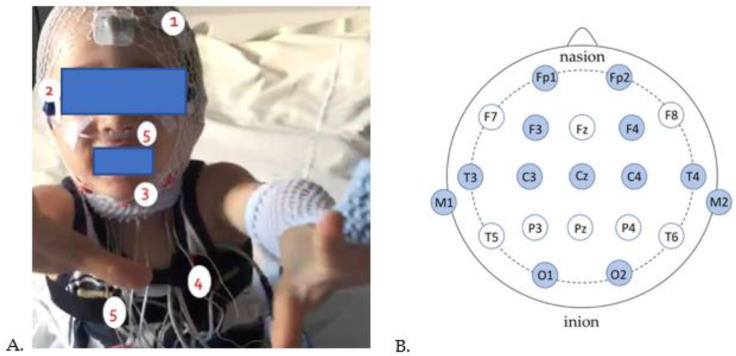
This prospective pilot study evaluated PTSD, SD (insomnia, nightmares), and sleep-wake rhythms in 11 children with PTSD (aged 3-18), compared with the age and sex-matched control groups. Assessment of PTSD and subjective and objective measures of sleep and sleep-wake rhythms (questionnaires, 24-h in-laboratory video-polysomnography, 15-day at-home actigraphy recording) were performed between 1 and 6 months after the traumatic event.
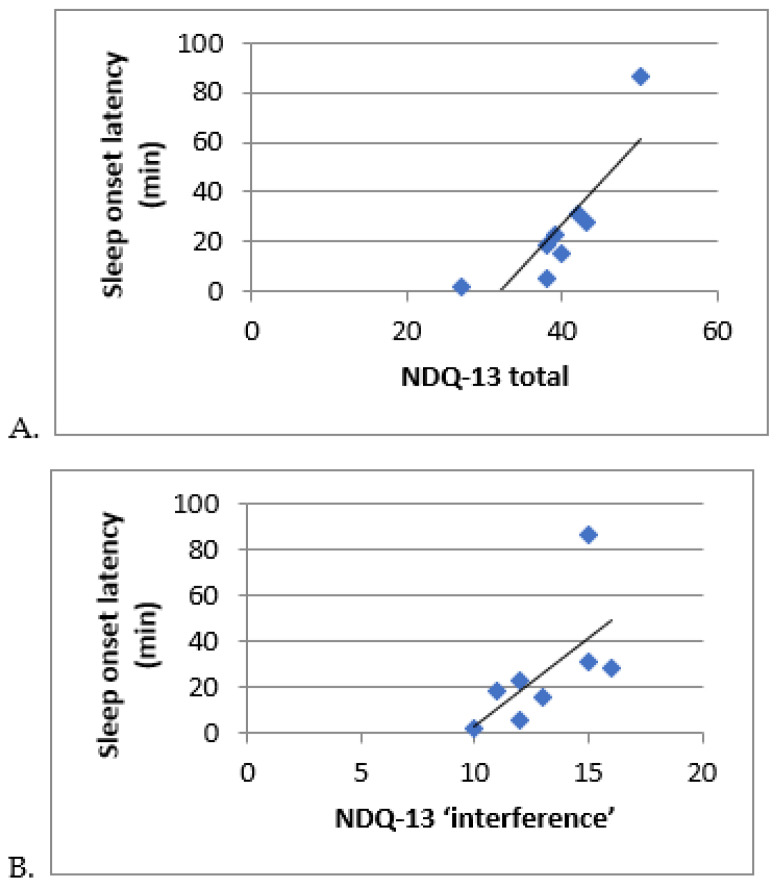
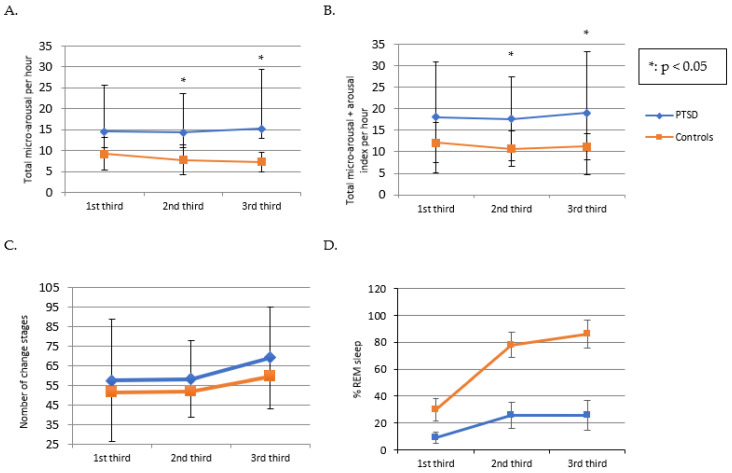
Children with PTSD had higher sleep fragmentation (increased wake-after-sleep onset, increased number of sleep stage changes) compared to controls, with a change in sleep microarchitecture (micro-arousal index at 14.8 versus 8.2, = 0.039). Sleep fragmentation parameters correlated with PTSD symptomatology, insomnia, and post-traumatic nightmare severity. The within-group comparison revealed a better sleep architecture in the controlled (sleep laboratory) than in the ecological condition (at home) (total sleep time 586 versus 464 min, = 0.018).
Sleep and rhythm disturbances are strongly associated with PTSD in children. The assessment of SD in children with PTSD should be carried out systematically and preferentially under ecological conditions, and management of SD should integrate the environment (environmental design, psycho-education for the children and their parents) more fully into therapy focused on sleep and trauma.
睡眠障碍(失眠和噩梦症状)是儿童创伤后应激障碍(PTSD)最敏感且持续存在的症状。若不进行治疗,这些与PTSD相关的睡眠障碍(SD)可预测PTSD的持续存在及精神并发症的增加。本研究的目的是在实验室和生态条件下,将PTSD儿童的睡眠和昼夜节律与对照人群进行比较,并首次检验SD和昼夜节律与PTSD严重程度及其共病呈正相关的假设。
这项前瞻性试点研究评估了11名PTSD儿童(年龄3 - 18岁)的PTSD、SD(失眠、噩梦)及睡眠 - 觉醒节律,并与年龄和性别匹配的对照组进行比较。在创伤事件发生后1至6个月,对PTSD以及睡眠和睡眠 - 觉醒节律的主观和客观指标(问卷、24小时实验室视频多导睡眠图、15天家庭活动记录仪记录)进行评估。
与对照组相比,PTSD儿童的睡眠碎片化程度更高(睡眠开始后觉醒增加、睡眠阶段变化次数增加),睡眠微结构发生改变(微觉醒指数为14.8对8.2,P = 0.039)。睡眠碎片化参数与PTSD症状、失眠及创伤后噩梦严重程度相关。组内比较显示,在受控(睡眠实验室)条件下的睡眠结构优于生态条件(在家中)(总睡眠时间586分钟对464分钟,P = 0.018)。
睡眠和节律紊乱与儿童PTSD密切相关。对于PTSD儿童的SD评估应系统地进行,且优先在生态条件下进行,SD的管理应将环境(环境设计、对儿童及其父母的心理教育)更全面地纳入以睡眠和创伤为重点的治疗中。