Department of Surgery, University of Michigan, Ann Arbor, MI.
Department of Surgery, Lake Washington Vascular Surgeons, Bellevue, WA.
J Vasc Surg Venous Lymphat Disord. 2024 Mar;12(2):101700. doi: 10.1016/j.jvsv.2023.101700. Epub 2023 Nov 11.
Effective treatment options are available for chronic venous insufficiency associated with superficial venous reflux. Although many patients with C2 and C3 disease based on the CEAP (Clinical-Etiological-Anatomical-Pathophysiological) classification have combined great saphenous vein (GSV) and saphenofemoral junction (SFJ) reflux, some may not have concomitant SFJ reflux. Several payors have determined that symptom severity in patients without SFJ reflux does not warrant treatment. In patients planned for venous ablation, we tested whether Venous Clinical Severity Scores (VCSS) are equivalent in those with GSV reflux alone compared with those with both GSV and SFJ reflux.
This cross-sectional study was conducted at 10 centers. Inclusion criteria were: candidate for endovenous ablation as determined by treating physician; 18 to 80 years of age; GSV reflux with or without SFJ reflux on ultrasound; and C2 or C3 disease. Exclusion criteria were prior deep vein thrombosis; prior vein ablation on the index limb; ilio-caval obstruction; and renal, hepatic, or heart failure requiring prior hospitalization. An a priori sample size was calculated. We used multiple linear regression (adjusted for patient characteristics) to compare differences in VCSS scores of the two groups at baseline, and to test whether scores were equivalent using a priori equivalence boundaries of +1 and -1. In secondary analyses, we tested differences in VCSS scores in patients with C2 and C3 disease separately.
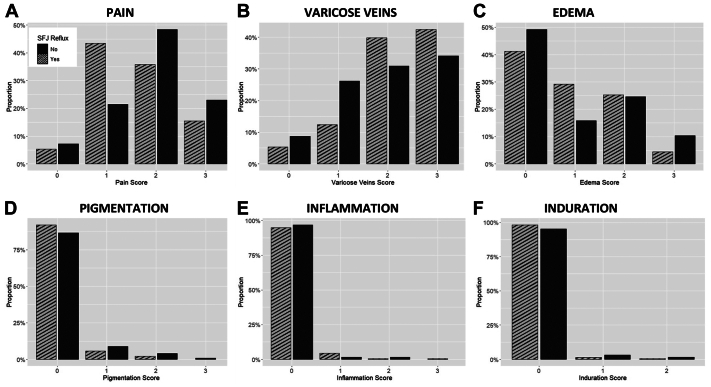
A total of 352 patients were enrolled; 64.2% (n = 226) had SFJ reflux, and 35.8% (n = 126) did not. The two groups did not differ by major clinical characteristics. The mean age of the cohort was 53.9 ± 14.3 years; women comprised 74.2%; White patients 85.8%; and body mass index was 27.8 ± 6.1 kg/m. The VCSS scores in patients with and without SFJ reflux were found to be equivalent; SFJ reflux was not a significant predictor of VCSS score; and mean VCSS scores did not differ significantly (6.4 vs 6.6, respectively, P = .40). In secondary subset analyses, VCSS scores were equivalent between C2 patients with and without SFJ reflux, and VCSS scores of C3 patients with SFJ reflux were lower than those without SFJ reflux.
Symptom severity is equivalent in patients with GSV reflux with or without SFJ reflux. The absence of SFJ reflux alone should not determine the treatment paradigm in patients with symptomatic chronic venous insufficiency. Patients with GSV reflux who meet clinical criteria for treatment should have equivalent treatment regardless of whether or not they have SFJ reflux.
对于伴有浅静脉反流的慢性静脉功能不全,有有效的治疗方法可供选择。虽然基于 CEAP(临床病因解剖病理生理)分类的 C2 和 C3 疾病的许多患者存在大隐静脉(GSV)和隐股交界处(SFJ)反流,但有些患者可能不存在同时存在 SFJ 反流。一些付款人已经确定,没有 SFJ 反流的患者的症状严重程度不需要治疗。对于计划进行静脉消融的患者,我们检测了在仅存在 GSV 反流的患者中,静脉临床严重程度评分(VCSS)是否与同时存在 GSV 和 SFJ 反流的患者相当。
这是一项在 10 个中心进行的横断面研究。纳入标准为:治疗医生确定适合静脉内消融的患者;年龄 18 至 80 岁;超声检查显示 GSV 反流伴或不伴 SFJ 反流;C2 或 C3 疾病。排除标准为:深静脉血栓形成史;指数肢体上先前的静脉消融;髂股静脉阻塞;以及需要先前住院治疗的肾功能、肝功能或心力衰竭。进行了预先计算样本量。我们使用多元线性回归(根据患者特征进行调整)比较了两组基线时 VCSS 评分的差异,并使用预先设定的等效边界+1 和-1 来测试评分是否等效。在次要分析中,我们分别测试了 C2 和 C3 疾病患者的 VCSS 评分差异。
共纳入 352 例患者;64.2%(n=226)存在 SFJ 反流,35.8%(n=126)不存在。两组在主要临床特征方面没有差异。队列的平均年龄为 53.9±14.3 岁;女性占 74.2%;白人患者占 85.8%;体重指数为 27.8±6.1kg/m。存在和不存在 SFJ 反流的患者的 VCSS 评分被发现是等效的;SFJ 反流不是 VCSS 评分的显著预测因子;平均 VCSS 评分差异无统计学意义(分别为 6.4 与 6.6,P=0.40)。在次要亚组分析中,C2 患者中存在和不存在 SFJ 反流的 VCSS 评分是等效的,而存在 SFJ 反流的 C3 患者的 VCSS 评分低于不存在 SFJ 反流的患者。
伴有 GSV 反流和不伴有 SFJ 反流的患者的症状严重程度是等效的。单独存在 SFJ 反流不应该决定有症状的慢性静脉功能不全患者的治疗模式。符合治疗临床标准的 GSV 反流患者,无论是否存在 SFJ 反流,都应接受等效的治疗。