Division of HIV, Infectious Diseases & Global Medicine, University of California San Francisco, San Francisco, CA, USA.
Division of HIV, Infectious Diseases & Global Medicine, University of California San Francisco, San Francisco, CA, USA.
Lancet Glob Health. 2023 Dec;11(12):e1899-e1910. doi: 10.1016/S2214-109X(23)00436-9.
Alcohol use is common among people with HIV and is a risk factor for tuberculosis disease and non-adherence to isoniazid preventive therapy (IPT). Few interventions exist to reduce alcohol use and increase IPT adherence in sub-Saharan Africa. The aim of this study was to test the hypothesis that financial incentives conditional on point-of-care negative urine alcohol biomarker testing and positive urine isoniazid testing would reduce alcohol use and increase isoniazid adherence, respectively, in people with HIV who have latent tuberculosis infection and hazardous alcohol use.
We conducted an open-label, 2×2 factorial randomised controlled trial in Uganda. Eligible for the study were non-pregnant HIV-positive adults (aged ≥18 years) prescribed antiretroviral therapy for at least 6 months, with current heavy alcohol use confirmed by urine ethyl glucuronide (biomarker of recent alcohol use) and a positive Alcohol Use Disorders Identification Test-Consumption (AUDIT-C; ≥3 for women, ≥4 for men) for the past 3 months' drinking, no history of active tuberculosis, tuberculosis treatment, or tuberculosis preventive therapy, and a positive tuberculin skin test. We randomly assigned participants (1:1:1:1) initiating 6 months of IPT to: no incentives (group 1); or incentives for recent alcohol abstinence (group 2), isoniazid adherence (group 3), or both (group 4). Escalating incentives were contingent on monthly point-of-care urine tests negative for ethyl glucuronide (groups 2 and 4), or positive on IsoScreen (biomarker of recent isoniazid use; groups 3 and 4). The primary alcohol outcome was non-hazardous use by self-report (AUDIT-C <3 for women, <4 for men) and phosphatidylethanol (PEth; past-month alcohol biomarker) <35 ng/mL at 3 months and 6 months. The primary isoniazid adherence outcome was more than 90% bottle opening of days prescribed. We performed intention-to-treat analyses. This trial is registered with ClinicalTrials.gov (NCT03492216), and is complete.
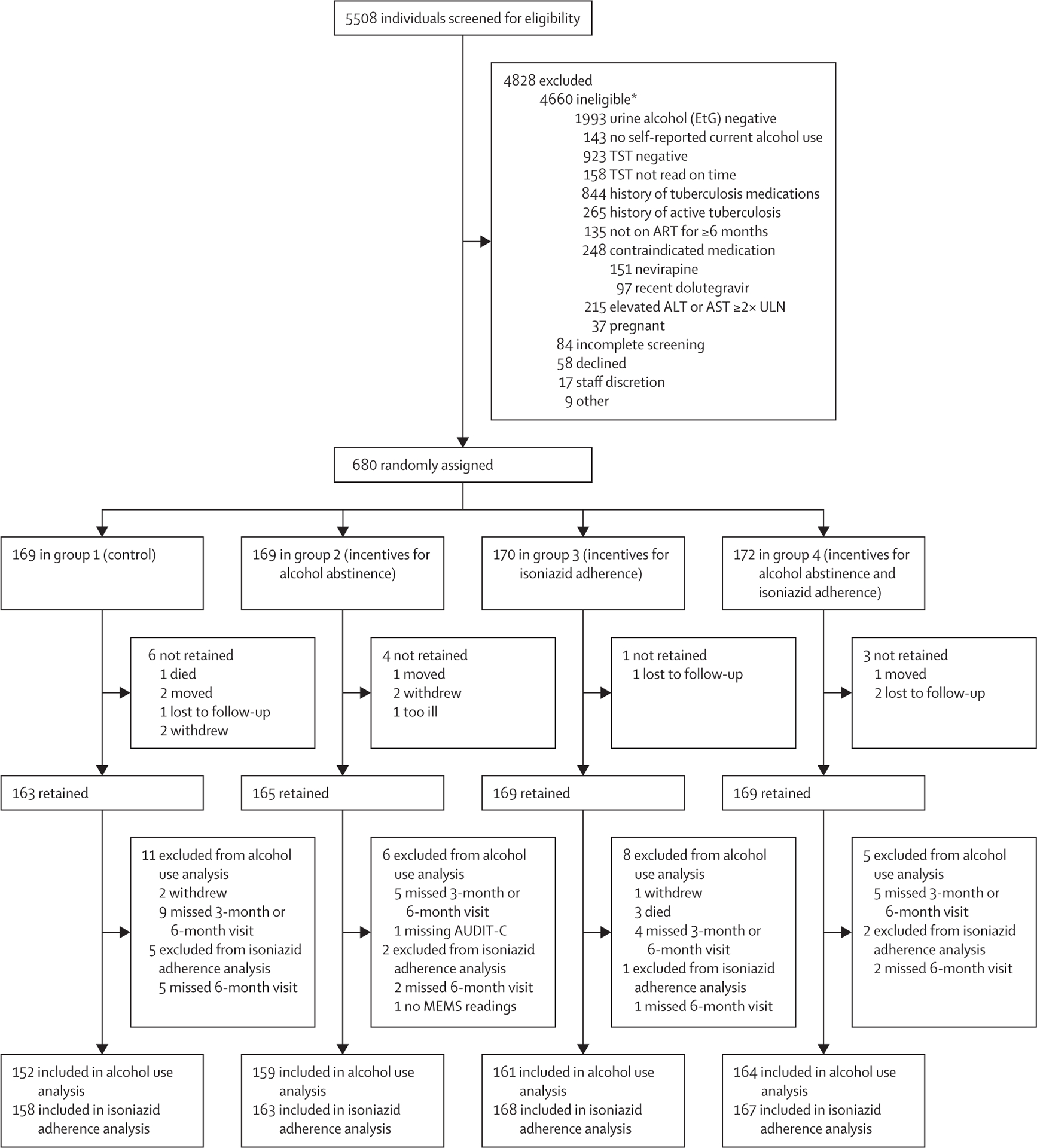
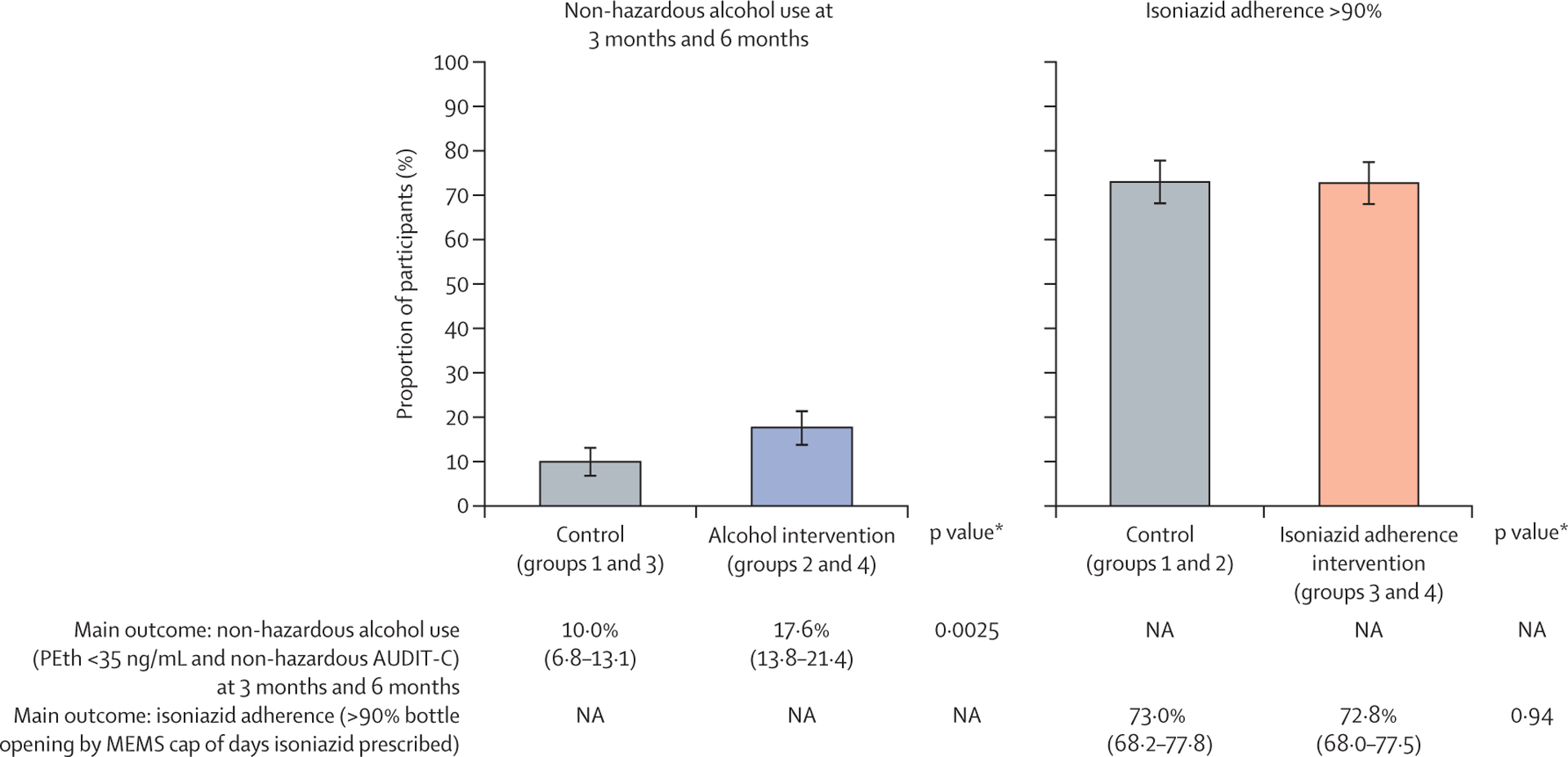
From April 16, 2018, to Aug 2, 2021, 5508 people were screened, of whom 680 were randomly assigned: 169 to group 1, 169 to group 2, 170 to group 3, and 172 to group 4. The median age of participants was 39 years (IQR 32-47), 470 (69%) were male, 598 (90%) of 663 had HIV RNA viral loads of less than 40 copies per mL, median AUDIT-C score was 6 (IQR 4-8), and median PEth was 252 ng/mL (IQR 87-579). Among 636 participants who completed the trial with alcohol use endpoint measures (group 1: 152, group 2: 159, group 3: 161, group 4: 164), non-hazardous alcohol use was more likely in the groups with incentives for alcohol abstinence (groups 2 and 4) versus no alcohol incentives (groups 1 and 3): 57 (17·6%) of 323 versus 31 (9·9%) of 313, respectively; adjusted risk difference (aRD) 7·6% (95% CI 2·7 to 12·5, p=0·0025). Among 656 participants who completed the trial with isoniazid adherence endpoint measures (group 1: 158, group 2: 163, group 3: 168, group 4: 167), incentives for isoniazid adherence did not increase adherence: 244 (72·8%) of 335 in the isoniazid incentive groups (groups 3 and 4) versus 234 (72·9%) of 321 in the no isoniazid incentive groups (groups 1 and 2); aRD -0·2% (95% CI -7·0 to 6·5, p=0·94). Overall, 53 (8%) of 680 participants discontinued isoniazid due to grade 3 or higher adverse events. There was no significant association between randomisation group and hepatotoxicity resulting in isoniazid discontinuation, after adjusting for sex and site.
Escalating financial incentives contingent on recent alcohol abstinence led to significantly lower biomarker-confirmed alcohol use versus control, but incentives for recent isoniazid adherence did not lead to changes in adherence. The alcohol intervention was efficacious despite less intensive frequency of incentives and clinic visits than traditional programmes for substance use, suggesting that pragmatic modifications of contingency management for resource-limited settings can have efficacy and that further evaluation of implementation is merited.
National Institute on Alcohol Abuse and Alcoholism.
For the Runyankole translation of the abstract see Supplementary Materials section.
在 HIV 感染者中,饮酒较为常见,且是结核病发病和异烟肼预防性治疗(IPT)依从性差的一个风险因素。在撒哈拉以南非洲,很少有干预措施可以减少饮酒量和提高 IPT 依从性。本研究旨在检验如下假设,即基于即时护理点阴性尿液酒精生物标志物检测和阳性尿液异烟肼检测结果提供经济激励,可分别减少 HIV 潜伏性结核感染和高危饮酒者的饮酒量,并提高其异烟肼依从性。
我们在乌干达开展了一项开放性、2×2 析因随机对照试验。合格入组者为正在接受至少 6 个月抗逆转录病毒治疗的非妊娠 HIV 阳性成年人,最近的尿液乙基葡萄糖醛酸(最近饮酒的生物标志物)和过去 3 个月内阳性的酒精使用障碍识别测试-饮酒量(女性≥3 分,男性≥4 分)证实存在大量饮酒,无活动性结核病、结核病治疗或结核病预防性治疗史,且结核菌素皮肤试验阳性。我们将参与者(1:1:1:1)随机分配到开始 6 个月 IPT 组:无激励组(第 1 组);或近期戒酒激励组(第 2 组)、异烟肼依从性激励组(第 3 组)或两者兼具激励组(第 4 组)。递增激励取决于每月即时护理点阴性尿液乙基葡萄糖醛酸检测(第 2 组和第 4 组),或阳性 IsoScreen(最近异烟肼使用的生物标志物;第 3 组和第 4 组)。主要饮酒结局是通过自我报告(女性 AUDIT-C<3 分,男性<4 分)和磷脂酰乙醇(过去 1 个月的酒精生物标志物)<35ng/ml 来评估,分别在 3 个月和 6 个月时评估。主要异烟肼依从性结局是按规定剂量打开药瓶的天数超过 90%。我们进行了意向治疗分析。这项试验在 ClinicalTrials.gov(NCT03492216)注册,现已完成。
从 2018 年 4 月 16 日至 2021 年 8 月 2 日,共筛选了 5508 人,其中 680 人被随机分配:第 1 组 169 人,第 2 组 169 人,第 3 组 170 人,第 4 组 172 人。参与者的中位年龄为 39 岁(IQR 32-47),470 人(69%)为男性,598 人(90%)的 HIV RNA 病毒载量低于 40 拷贝/ml,中位 AUDIT-C 评分为 6 分(IQR 4-8),中位磷脂酰乙醇水平为 252ng/ml(IQR 87-579)。在完成酒精使用终点测量的 636 名参与者中(第 1 组:152 名,第 2 组:159 名,第 3 组:161 名,第 4 组:164 名),与无酒精激励组(第 1 组和第 3 组)相比,有酒精激励组(第 2 组和第 4 组)的非危险饮酒可能性更高:分别有 57(17.6%)和 31(9.9%)人,调整后的风险差异(aRD)为 7.6%(95%CI 2.7-12.5,p=0.0025)。在完成异烟肼依从性终点测量的 656 名参与者中(第 1 组:158 名,第 2 组:163 名,第 3 组:168 名,第 4 组:167 名),异烟肼依从性激励并未增加依从性:在有激励组(第 3 组和第 4 组)中,244 人(72.8%),而在无激励组(第 1 组和第 2 组)中,234 人(72.9%),aRD 为-0.2%(95%CI -7.0-6.5,p=0.94)。总体而言,由于出现 3 级或更高级别的不良事件,680 名参与者中有 53 人(8%)停止服用异烟肼。在调整了性别和地点后,随机分组与导致异烟肼停药的肝毒性之间没有显著关联。
基于最近戒酒情况的递增经济激励与生物标志物证实的饮酒量减少显著相关,但近期异烟肼依从性的激励并未导致依从性的改变。尽管与传统物质使用方案相比,该酒精干预措施的激励频率和就诊次数较少,但仍具有疗效,表明资源有限环境下的Contingency Management 可以进行务实的修改,并值得进一步评估实施情况。
美国国家酗酒与酒精中毒研究所。