Rudin Charles M, Liu Stephen V, Soo Ross A, Lu Shun, Hong Min Hee, Lee Jong-Seok, Bryl Maciej, Dumoulin Daphne W, Rittmeyer Achim, Chiu Chao-Hua, Ozyilkan Ozgur, Johnson Melissa, Navarro Alejandro, Novello Silvia, Ozawa Yuichi, Tam Sammi Hiu, Patil Namrata S, Wen Xiaohui, Huang Meilin, Hoang Tien, Meng Raymond, Reck Martin
Memorial Sloan Kettering Cancer Center, New York, NY.
Georgetown University, Washington, DC.
J Clin Oncol. 2024 Jan 20;42(3):324-335. doi: 10.1200/JCO.23.01363. Epub 2023 Nov 17.
The phase III SKYSCRAPER-02 study determined whether the benefits of atezolizumab plus carboplatin and etoposide (CE) could be enhanced by the addition of tiragolumab in untreated extensive-stage small-cell lung cancer (ES-SCLC). We report final progression-free survival (PFS) and overall survival (OS) analyses.
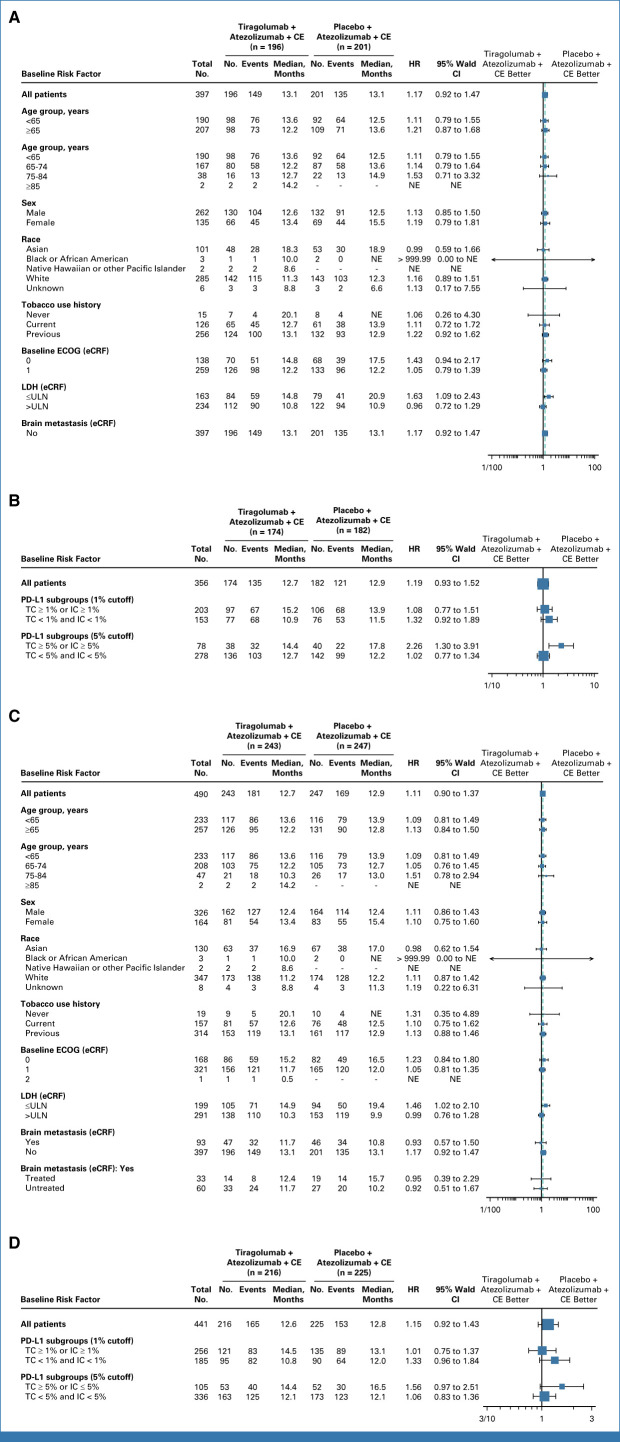
Patients received tiragolumab 600 mg/placebo, plus atezolizumab 1,200 mg and CE (four cycles), then maintenance tiragolumab/placebo plus atezolizumab. Primary end points were investigator-assessed PFS and OS in patients without history/presence of brain metastases (primary analysis set [PAS]). Additional end points included PFS and OS in all patients regardless of brain metastases status (full analysis set [FAS]), response, and safety.
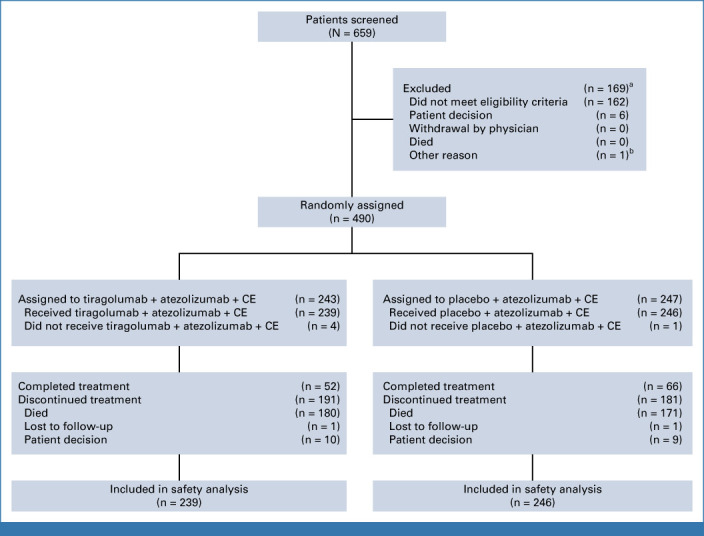
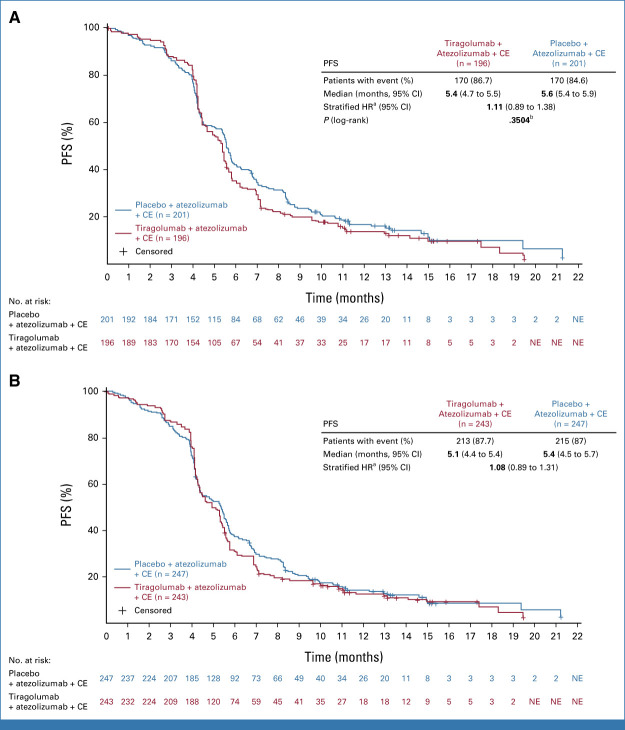
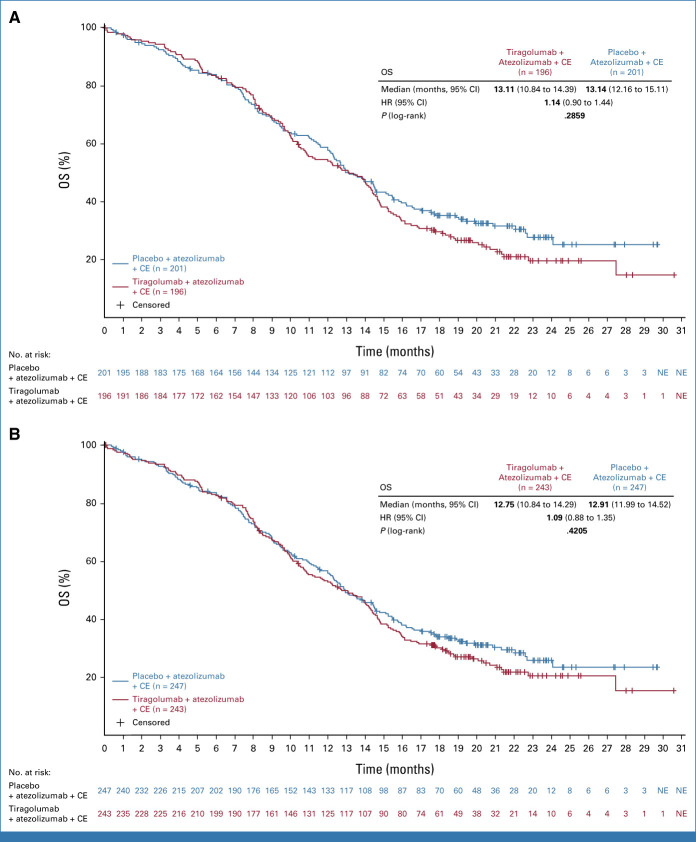
Four hundred ninety patients were randomly assigned (FAS): 243 to tiragolumab arm and 247 to control arm. At the cutoff date (February 6, 2022; median duration of follow-up, 14.3 months [PAS] and 13.9 months [FAS]), final analysis of PFS in the PAS (n = 397) did not reach statistical significance (stratified hazard ratio [HR], 1.11; = .3504; median, 5.4 months tiragolumab 5.6 months control). At the cutoff date (September 6, 2022; median duration of follow-up, 21.2 months [FAS]), median OS in the PAS at final OS analysis was 13.1 months in both arms (stratified HR, 1.14; = .2859). Median PFS and OS in the FAS were consistent with the PAS. The proportion of patients with immune-mediated adverse events (AEs) in the tiragolumab and control arms was 54.4% and 49.2%, respectively (grade 3/4: 7.9% and 7.7%). AEs leading to treatment withdrawal occurred in 8.4% and 9.3% of tiragolumab- and control-treated patients, respectively.
Tiragolumab did not provide additional benefit over atezolizumab and CE in untreated ES-SCLC. The combination was well tolerated with no new safety signals.
III期SKYSCRAPER-02研究确定了在未经治疗的广泛期小细胞肺癌(ES-SCLC)中,添加替雷戈珠单抗是否能增强阿替利珠单抗联合卡铂和依托泊苷(CE)的疗效。我们报告了最终的无进展生存期(PFS)和总生存期(OS)分析结果。
患者接受600mg替雷戈珠单抗/安慰剂,加1200mg阿替利珠单抗和CE(四个周期),然后接受替雷戈珠单抗/安慰剂加阿替利珠单抗维持治疗。主要终点是研究者评估的无脑转移病史/存在脑转移患者的PFS和OS(主要分析集[PAS])。其他终点包括所有患者(无论脑转移状态如何)的PFS和OS(全分析集[FAS])、缓解率和安全性。
490例患者被随机分组(FAS):243例进入替雷戈珠单抗组,247例进入对照组。在截止日期(2022年2月6日;中位随访时间,PAS为14.3个月,FAS为13.9个月),对PAS中397例患者的PFS进行的最终分析未达到统计学显著性(分层风险比[HR],1.11;P = 0.3504;中位值,替雷戈珠单抗组为5.4个月,对照组为5.6个月)。在截止日期(2022年9月6日;中位随访时间,FAS为21.2个月),最终OS分析时PAS中两组的中位OS均为13.1个月(分层HR,1.14;P = 0.2859)。FAS中的中位PFS和OS与PAS一致。替雷戈珠单抗组和对照组中发生免疫介导不良事件(AE)的患者比例分别为54.4%和49.2%(3/4级:7.9%和7.7%)。因AE导致治疗中断的情况分别发生在8.4%接受替雷戈珠单抗治疗的患者和9.3%接受对照治疗的患者中。
在未经治疗的ES-SCLC中,替雷戈珠单抗相比阿替利珠单抗联合CE未提供额外益处。该联合方案耐受性良好,无新的安全信号。