Microbiology and Virology Unit, University Hospital Città Della Salute E Della Scienza Di Torino, Corso Bramante 88/90, 10126, Turin, Italy.
Department of Public Health and Paediatrics, University of Torino, Turin, Italy.
Eur J Clin Microbiol Infect Dis. 2024 Jan;43(1):155-166. doi: 10.1007/s10096-023-04712-8. Epub 2023 Nov 21.
Ceftazidime/avibactam-resistance in Klebsiella pneumoniae carbapenemase-producing Klebsiella pneumoniae (KPC-Kp) is a topic of great interest for epidemiological, diagnostic, and therapeutical reasons. However, data on its prevalence and burden on mortality in patients with bloodstream infection (BSI) are lacking. This study was aimed at identifying risk factors for mortality in patients suffering from ceftazidime/avibactam-resistant KPC-Kp BSI.
An observational retrospective study (January 2018-December 2022) was conducted at a tertiary hospital including all consecutive hospitalized adult patients with a ceftazidime/avibactam-resistant KPC-Kp BSI. Data on baseline clinical features, management, and admission outcomes were analyzed.
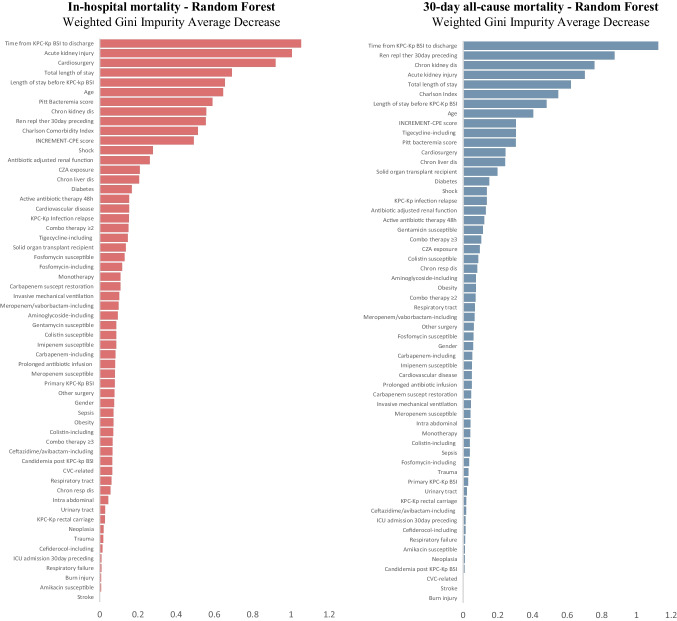
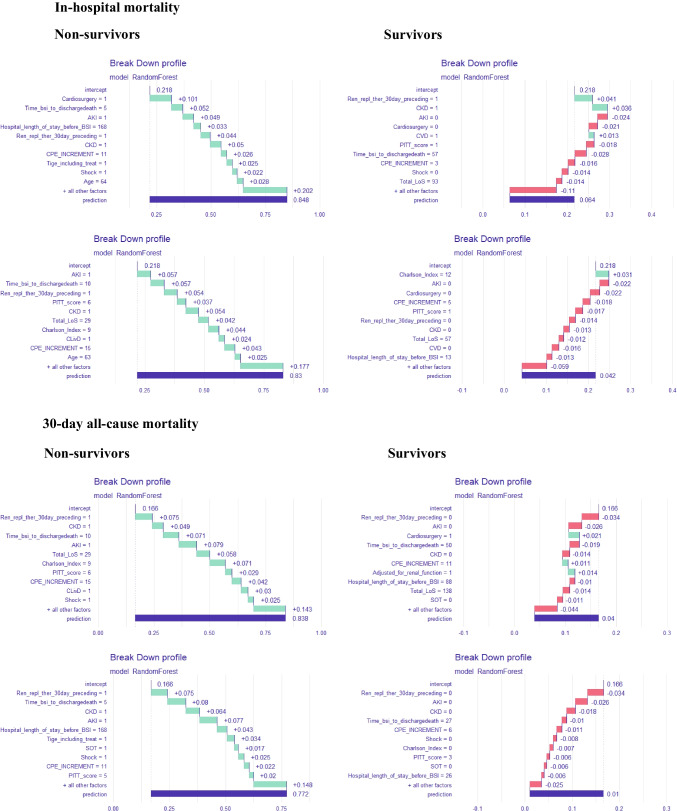
Over the study period, among all the KPC-Kp BSI events recorded, 38 (10.5%) were caused by ceftazidime/avibactam-resistant KPC-Kp strains, 37 events being finally included. The ceftazidime/avibactam-resistant KPC-Kp strains revealed susceptibility restoration to at least one carbapenem in more than 60% of cases. In-hospital and 30-day all-cause mortality rates were 22% and 16.2%, respectively. Non-survivors suffered from more baseline comorbidities and experienced a more severe ceftazidime/avibactam-resistant KPC-Kp BSI presentation (i.e., both the Pitt Bacteremia and INCREMENT-CPE scores were significantly higher). Presenting with a higher Charlson Comorbidity Index, chronic kidney disease-KDIGO stage 3A or worse-having recently gone through renal replacement therapy, having suffered from an acute kidney injury following the ceftazidime/avibactam-resistant KPC-Kp BSI, and being admitted for cardiac surgery were the strongest predictors of mortality.
Ceftazidime/avibactam resistance in KPC-Kp BSI easily emerged in our highly KPC-Kp endemic area with remarkable mortality rates. Our findings might provide physicians possibly actionable information when managing patients with a ceftazidime/avibactam-resistant KPC-Kp BSI.
产碳青霉烯酶肺炎克雷伯菌(KPC-Kp)对头孢他啶/阿维巴坦的耐药性是一个具有重要流行病学、诊断和治疗意义的话题。然而,关于其在血流感染(BSI)患者中的流行率和死亡率负担的数据尚缺乏。本研究旨在确定患有头孢他啶/阿维巴坦耐药 KPC-Kp BSI 的患者死亡的危险因素。
一项观察性回顾性研究(2018 年 1 月至 2022 年 12 月)在一家三级医院进行,纳入所有连续住院的成人头孢他啶/阿维巴坦耐药 KPC-Kp BSI 患者。分析了基线临床特征、治疗和入院结局的数据。
在研究期间,在所记录的所有 KPC-Kp BSI 事件中,38 例(10.5%)由头孢他啶/阿维巴坦耐药 KPC-Kp 菌株引起,最终纳入 37 例事件。超过 60%的头孢他啶/阿维巴坦耐药 KPC-Kp 菌株对至少一种碳青霉烯类药物的敏感性恢复。院内和 30 天全因死亡率分别为 22%和 16.2%。非幸存者患有更多的基线合并症,且经历了更严重的头孢他啶/阿维巴坦耐药 KPC-Kp BSI 表现(即 Pitt 菌血症评分和 INCREMENT-CPE 评分均显著升高)。Charlson 合并症指数较高、慢性肾脏病-KDIGO 3A 期或更差、近期接受肾脏替代治疗、头孢他啶/阿维巴坦耐药 KPC-Kp BSI 后发生急性肾损伤以及因心脏手术入院是死亡的最强预测因素。
在我们高度流行 KPC-Kp 的地区,KPC-Kp BSI 中很容易出现头孢他啶/阿维巴坦耐药,且死亡率显著。我们的研究结果可能为医生在管理头孢他啶/阿维巴坦耐药 KPC-Kp BSI 患者时提供有用的信息。