Williams Adam R, Moya-Mendez Mary E, Mehta Sachin, Vekstein Andrew, Harrison J Kevin, Milano Carmelo A, Plichta Ryan P, Haney John, Schroder Jacob N, Zwischenberger Brittany, Glower Donald, Gaca Jeffrey G
Division of Cardiothoracic Surgery, Department of Surgery, Duke University Hospital, Durham, NC.
Division of Cardiothoracic Anesthesia, Department of Anesthesia, Duke University Hospital, Durham, NC.
JTCVS Tech. 2023 Aug 7;22:228-236. doi: 10.1016/j.xjtc.2023.07.022. eCollection 2023 Dec.
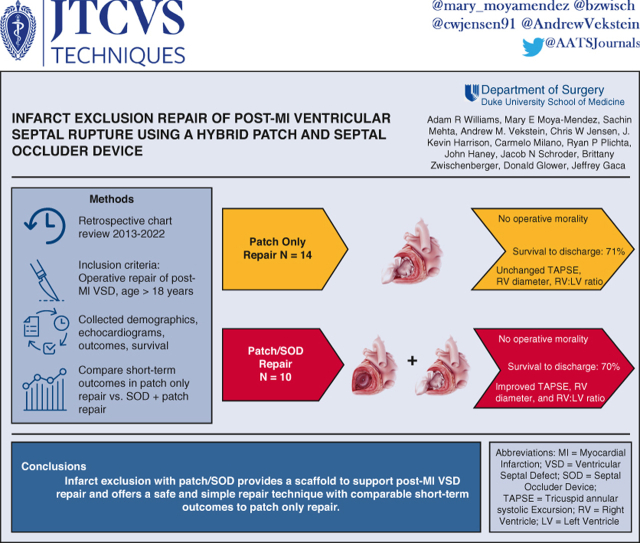
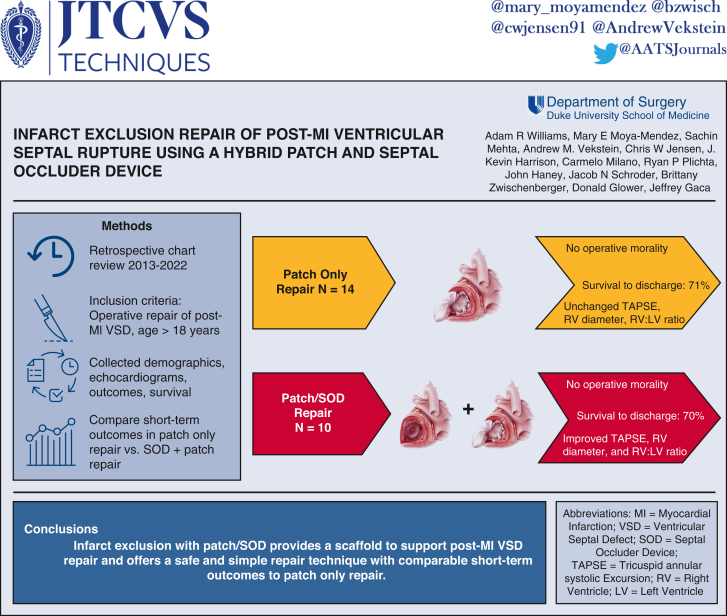
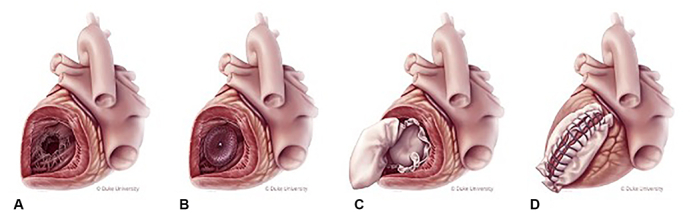
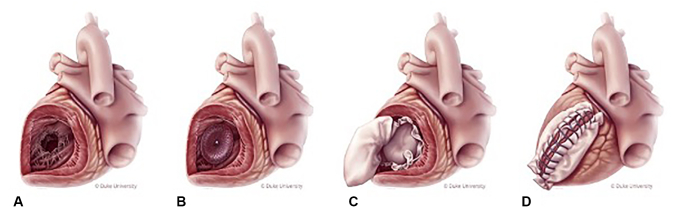
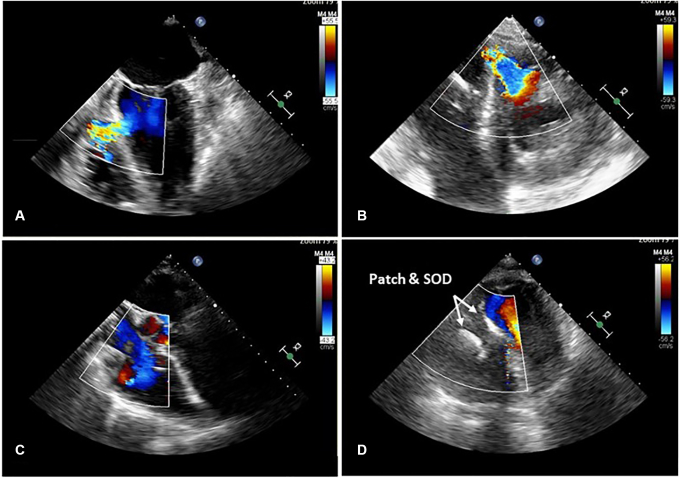
We developed a hybrid technique for repairing post-myocardial infarction (MI) ventricular septal defect (VSD) that combines infarct exclusion with patch and a nitinol-mesh septal occluder device (SOD) to provide a scaffold to support the damaged septal wall. Here, we compare outcomes of patients with post-MI VSD repaired using patch only or hybrid patch/SOD.
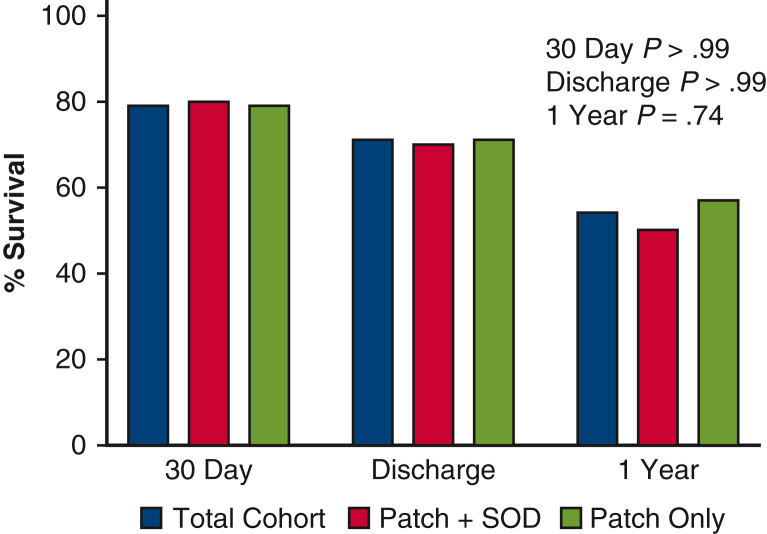
Patients undergoing post-MI VSD repair at our institution from 2013 to 2022 who received patch alone or patch/SOD repair were analyzed. Primary outcome was survival to hospital discharge. Clinical outcomes and echocardiograms were also analyzed.
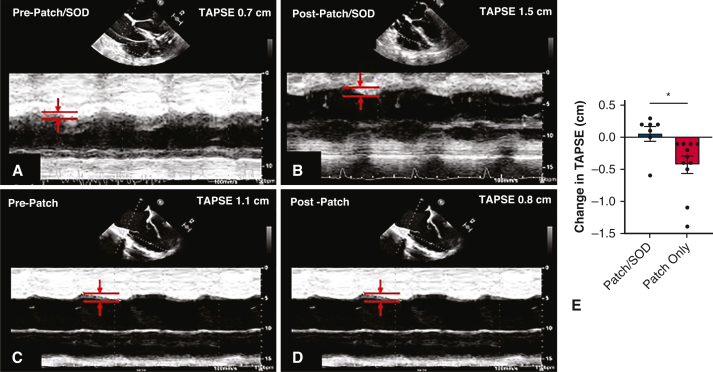
Over a 9-year period, 24 patients had post-MI VSD repair at our institution with either hybrid patch/SOD (n = 10) or patch only repair (n = 14). VSD size was 18 ± 5.8 mm for patch/SOD and 17 ± 4.6 mm for patch only. In the patch/SOD repair cohort, average size of SOD implant was 23.6 ± 5.6 mm. Mild left ventricular dysfunction was present prerepair and was unchanged postrepair in both groups; however, moderate-to-severe right ventricular (RV) dysfunction was common in both groups before repair. RV function worsened or persisted as severe in 10% of hybrid versus 54% of patch-only patients postrepair. Tricuspid annular systolic excursion and RV:left ventricle diameter ratio, quantitative metrics of RV function, improved after patch/SOD repair. No intraoperative mortality occurred in either group. Postoperative renal, hepatic, and respiratory failure requiring tracheostomy was common in both groups. Survival to hospital discharge in both cohorts was 70%.
Post-MI VSD repair with patch/SOD has comparable short-term outcomes with patch alone. Addition of a SOD to patch repair provides a scaffold that may enhance the repair of post-MI VSD with patch exclusion.
我们开发了一种用于修复心肌梗死后(MI)室间隔缺损(VSD)的混合技术,该技术将梗死灶切除术与补片以及镍钛合金网状间隔封堵器(SOD)相结合,以提供一个支架来支撑受损的间隔壁。在此,我们比较仅使用补片或补片/SOD混合修复的MI后VSD患者的结局。
分析了2013年至2022年在我们机构接受MI后VSD修复的患者,这些患者接受了单独补片或补片/SOD修复。主要结局是存活至出院。还分析了临床结局和超声心动图。
在9年期间,我们机构有24例患者接受了MI后VSD修复,其中采用补片/SOD混合修复(n = 10)或仅补片修复(n = 14)。补片/SOD组的VSD大小为18±5.8 mm,仅补片组为17±4.6 mm。在补片/SOD修复队列中,SOD植入物的平均大小为23.6±5.6 mm。两组在修复前均存在轻度左心室功能障碍,修复后无变化;然而,两组在修复前中度至重度右心室(RV)功能障碍均很常见。修复后,10%的混合修复患者与54%的仅补片修复患者的RV功能恶化或持续为重度。补片/SOD修复后,RV功能的定量指标三尖瓣环收缩期位移和RV与左心室直径比有所改善。两组均未发生术中死亡。两组术后均常见需要气管切开术的肾、肝和呼吸衰竭。两个队列的出院存活率均为70%。
补片/SOD修复MI后VSD的短期结局与仅用补片修复相当。在补片修复中添加SOD可提供一个支架,可能会增强通过补片切除术修复MI后VSD的效果。