Division of Behavioral Medicine and Neurosciences, Department of Psychiatry and Behavioral Sciences, Duke University Medical Center, Durham, North Carolina, USA.
Division of Cardiovascular and Thoracic Surgery, Department of Surgery, Duke University Medical Center, Durham, North Carolina, USA.
Ann Clin Transl Neurol. 2024 Feb;11(2):263-277. doi: 10.1002/acn3.51949. Epub 2023 Dec 28.
Although acute brain infarcts are common after surgical aortic valve replacement (SAVR), they are often unassociated with clinical stroke symptoms. The relationship between clinically "silent" infarcts and in-hospital delirium remains uncertain; obscured, in part, by how infarcts have been traditionally summarized as global metrics, independent of location or structural consequence. We sought to determine if infarct location and related structural connectivity changes were associated with postoperative delirium after SAVR.
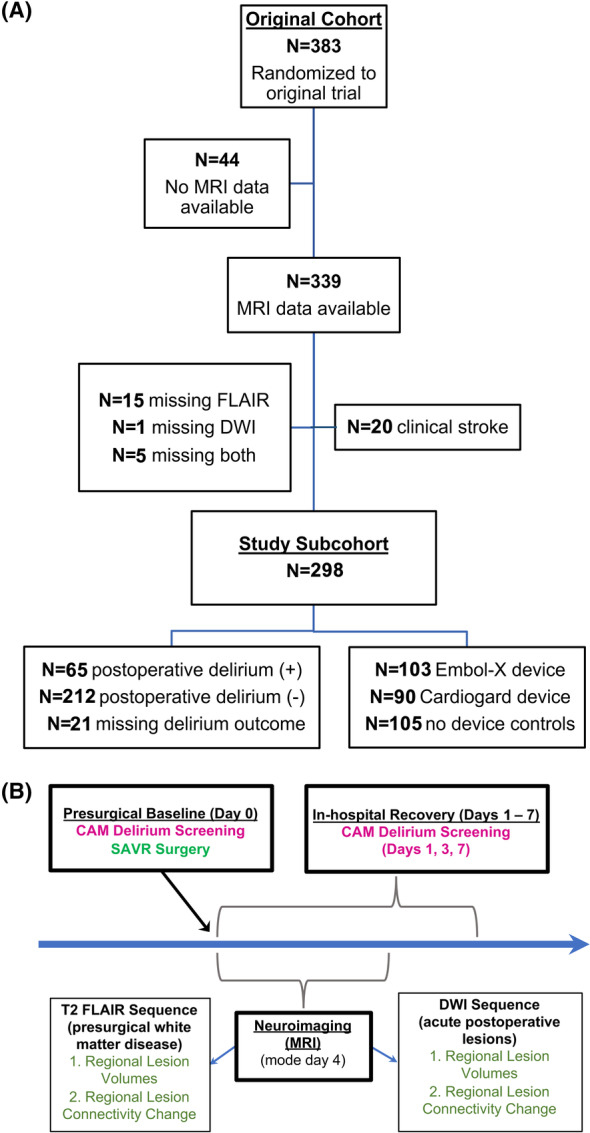
A secondary analysis of a randomized multicenter SAVR trial of embolic protection devices (NCT02389894) was conducted, excluding participants with clinical stroke or incomplete neuroimaging (N = 298; 39% female, 7% non-White, 74 ± 7 years). Delirium during in-hospital recovery was serially screened using the Confusion Assessment Method. Parcellation and tractography atlas-based neuroimaging methods were used to determine infarct locations and cortical connectivity effects. Mixed-effect, zero-inflated gaussian modeling analyses, accounting for brain region-specific infarct characteristics, were conducted to examine for differences within and between groups by delirium status and perioperative neuroprotection device strategy.
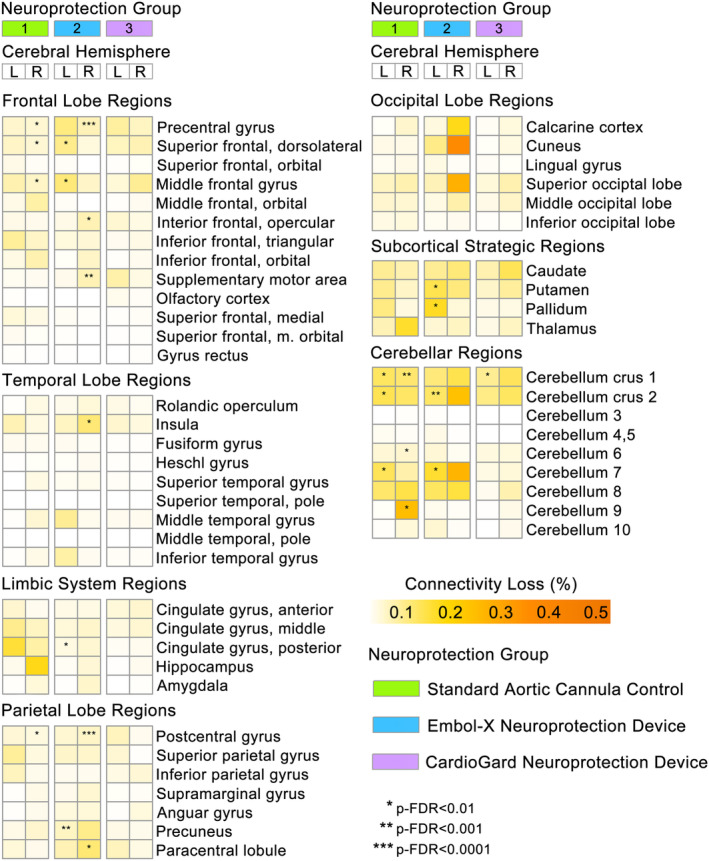
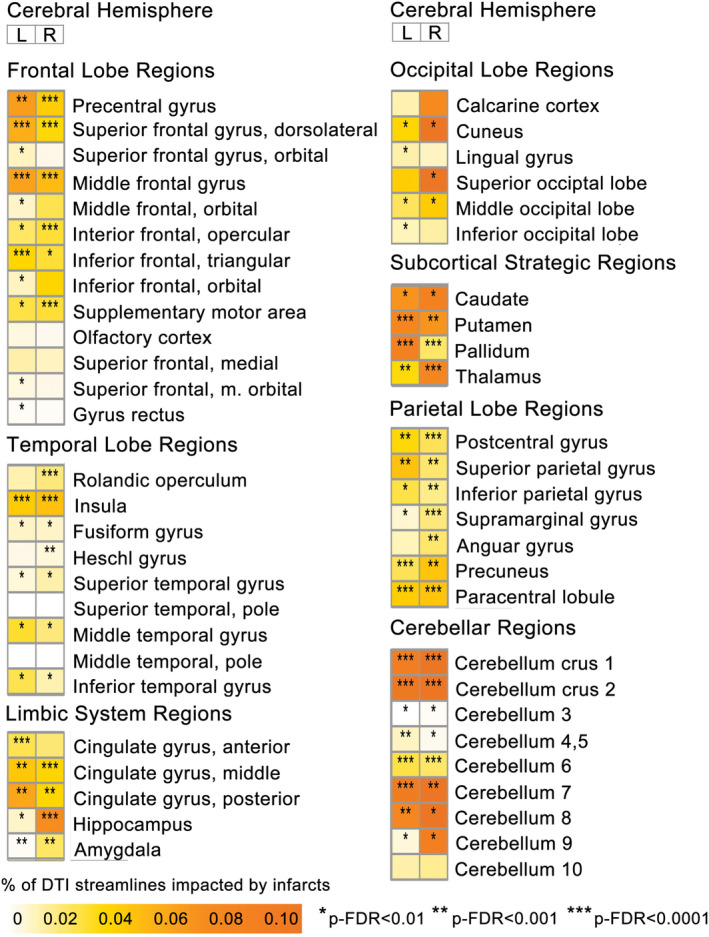
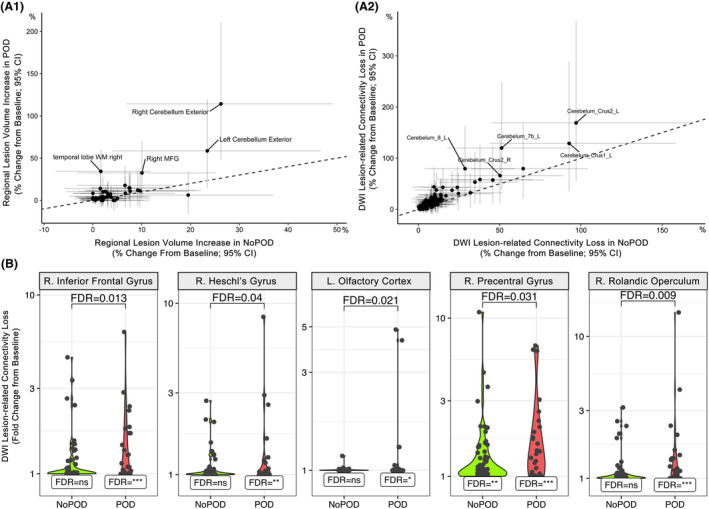
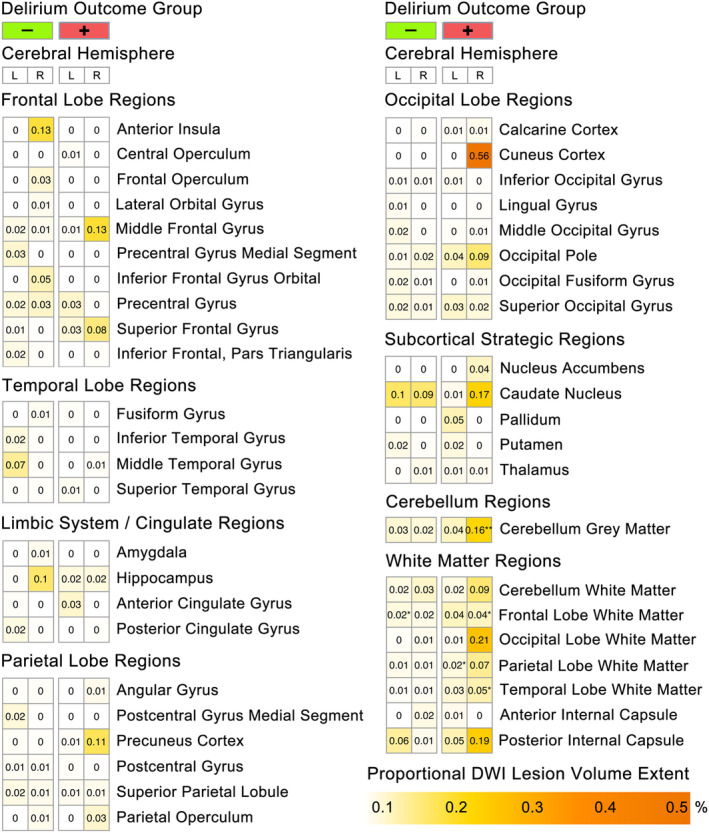
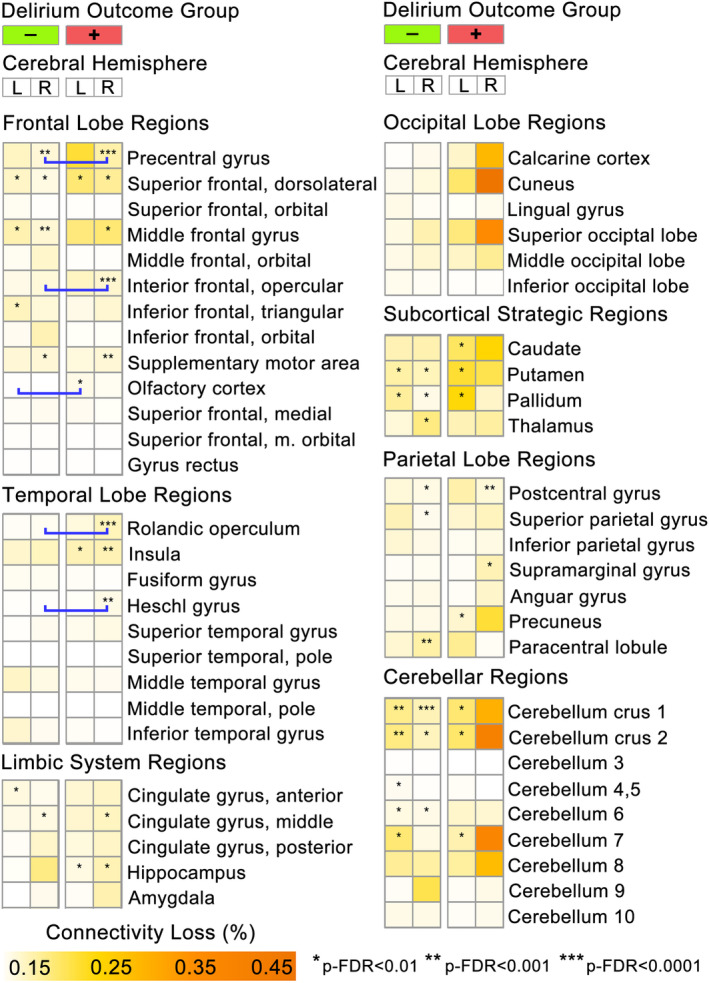
23.5% participants experienced postoperative delirium. Delirium was associated with significantly increased lesion volumes in the right cerebellum and temporal lobe white matter, while diffusion weighted imaging infarct-related structural disconnection (DWI-ISD) was observed in frontal and temporal lobe regions (p-FDR < 0.05). Fewer brain regions demonstrated DWI-ISD loss in the suction-based neuroprotection device group, relative to filtration-based device or standard aortic cannula.
Structural disconnection from acute infarcts was greater in patients who experienced postoperative delirium, suggesting that the impact from covert perioperative infarcts may not be as clinically "silent" as commonly assumed.
虽然外科主动脉瓣置换术(SAVR)后常发生急性脑梗死,但通常与临床中风症状无关。“无症状”梗死与住院期间谵妄之间的关系尚不确定;部分原因是梗死传统上被总结为全局指标,而不考虑位置或结构后果。我们试图确定 SAVR 后梗死部位及其相关结构连接变化是否与术后谵妄有关。
对一项使用栓塞保护装置的随机多中心 SAVR 试验(NCT02389894)进行二次分析,排除有临床中风或神经影像学不完整的参与者(N=298;39%为女性,7%为非白人,74±7岁)。使用意识模糊评估法(CAM)对住院期间恢复期间的谵妄进行连续筛查。使用分区和束追踪图谱基于神经影像学方法确定梗死部位和皮质连接影响。采用混合效应、零膨胀高斯模型分析,考虑到脑区特定梗死特征,对谵妄状态和围手术期神经保护装置策略的差异进行组内和组间分析。
23.5%的参与者发生术后谵妄。谵妄与右侧小脑和颞叶白质的病变体积明显增加有关,而弥散加权成像梗死相关结构分离(DWI-ISD)则见于额叶和颞叶区域(p-FDR<0.05)。与基于过滤的装置或标准主动脉插管相比,基于抽吸的神经保护装置组中,有更少的脑区出现 DWI-ISD 丢失。
术后发生谵妄的患者中,急性梗死的结构分离程度更大,这表明隐匿性围手术期梗死的影响可能并不像通常认为的那样“无症状”。