Department of Neonatal and Paediatric Intensive Care, Copenhagen University Hospital, Rigshospitalet, Copenhagen, Denmark.
Department of Clinical Medicine, University of Copenhagen, Copenhagen, Denmark.
Pediatr Res. 2024 Sep;96(4):1084-1089. doi: 10.1038/s41390-023-02998-0. Epub 2024 Jan 11.
Using pre-procedure analgesia with the risk of apnoea may complicate the Less Invasive Surfactant Administration (LISA) procedure or reduce the effect of LISA.
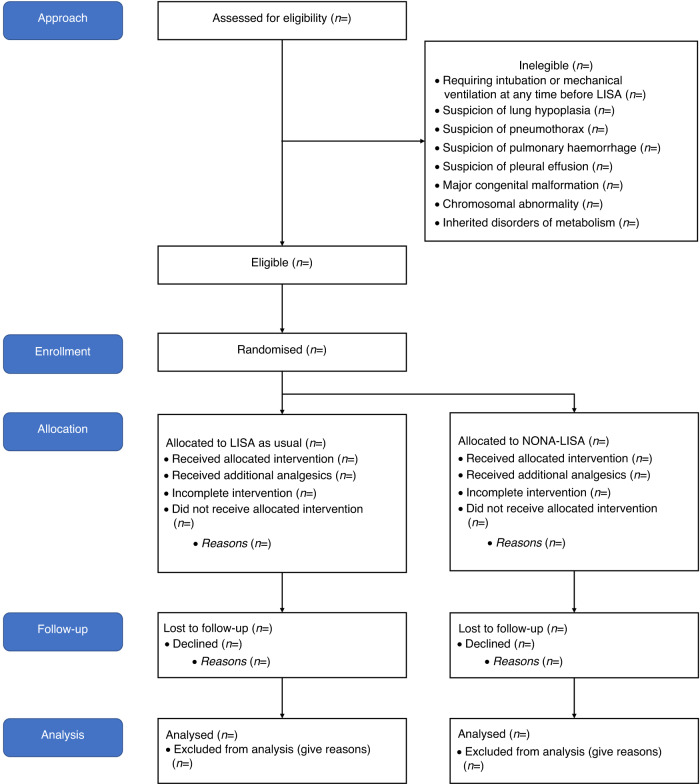
The NONA-LISA trial (ClinicalTrials.gov, NCT05609877) is a multicentre, blinded, randomised controlled trial aiming at including 324 infants born before 30 gestational weeks, meeting the criteria for surfactant treatment by LISA. Infants will be randomised to LISA after administration of fentanyl 0.5-1 mcg/kg intravenously (fentanyl group) or isotonic saline solution intravenously (saline group). All infants will receive standardised non-pharmacological comfort care before and during the LISA procedure. Additional analgesics will be provided at the clinician's discretion. The primary outcome is the need for invasive ventilation, meaning mechanical or manual ventilation via an endotracheal tube, for at least 30 min (cumulated) within 24 h of the procedure. Secondary outcomes include the modified COMFORTneo score during the procedure, bronchopulmonary dysplasia at 36 weeks, and mortality at 36 weeks.
The NONA-LISA trial has the potential to provide evidence for a standardised approach to relief from discomfort in preterm infants during LISA and to reduce invasive ventilation. The results may affect future clinical practice.
Pre-procedure analgesia is associated with apnoea and may complicate procedures that rely on regular spontaneous breathing, such as Less Invasive Surfactant Administration (LISA). This randomised controlled trial addresses the effect of analgesic premedication in LISA by comparing fentanyl with a placebo (isotonic saline) in infants undergoing the LISA procedure. All infants will receive standardised non-pharmacological comfort. The NONA-LISA trial has the potential to provide evidence for a standardised approach to relief from discomfort or pain in preterm infants during LISA and to reduce invasive ventilation. The results may affect future clinical practice regarding analgesic treatment associated with the LISA procedure.
使用有呼吸暂停风险的术前镇痛可能会使微创表面活性剂给药(LISA)程序复杂化或降低 LISA 的效果。
NONA-LISA 试验(ClinicalTrials.gov,NCT05609877)是一项多中心、盲法、随机对照试验,旨在纳入 324 名胎龄小于 30 周且符合 LISA 表面活性剂治疗标准的婴儿。婴儿将在静脉注射芬太尼 0.5-1mcg/kg(芬太尼组)或静脉注射等渗盐水溶液(盐水组)后随机接受 LISA 治疗。所有婴儿在 LISA 程序之前和期间将接受标准化的非药物性舒适护理。根据临床医生的判断,将提供额外的镇痛剂。主要结局是程序后 24 小时内至少需要 30 分钟(累积)的有创通气,即通过气管内管进行机械通气或手动通气。次要结局包括程序期间改良的 COMFORTneo 评分、36 周时支气管肺发育不良和 36 周时死亡率。
NONA-LISA 试验有可能为 LISA 期间缓解早产儿不适提供标准方法,并减少有创通气。结果可能会影响未来的临床实践。
术前镇痛与呼吸暂停有关,并且可能使依赖于正常自主呼吸的程序复杂化,例如微创表面活性剂给药(LISA)。这项随机对照试验通过比较芬太尼与安慰剂(等渗盐水)在接受 LISA 程序的婴儿中,研究了 LISA 中镇痛预给药的效果。所有婴儿将接受标准化的非药物性舒适护理。NONA-LISA 试验有可能为 LISA 期间缓解早产儿不适或疼痛提供标准方法,并减少有创通气。结果可能会影响未来与 LISA 程序相关的镇痛治疗的临床实践。