Weipert Kay F, Kostic Srdjan, Gökyildirim Timur, Johnson Victoria, Chasan Ritvan, Gemein Christopher, Rosenbauer Josef, Erkapic Damir, Schmitt Jörn
Department of Cardiology, Rhythmology and Angiology, Medizinische Klinik II, Diakonie Klinikum Jung Stilling, 57074 Siegen, Germany.
Department of Cardiology, Kantonsspital Aarau, 5001 Aarau, Switzerland.
J Clin Med. 2023 Dec 26;13(1):129. doi: 10.3390/jcm13010129.
The use of the S-ICD is limited by its inability to provide backup pacing. Combined use of the S-ICD with a pacemaker may be a good choice in certain situations, yet current experience concerning the compatibility is limited. The goal of this study was to determine the safety and efficacy of the S-ICD in patients with a pacemaker.
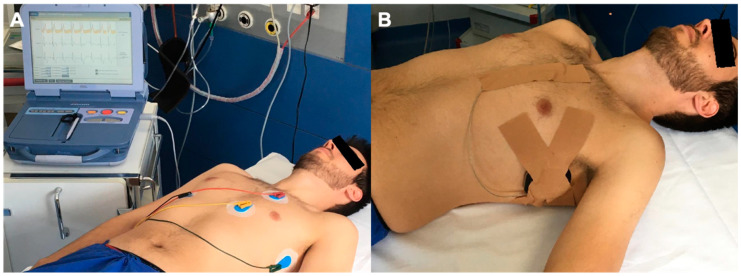
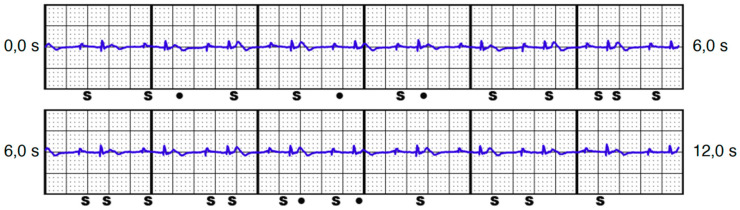
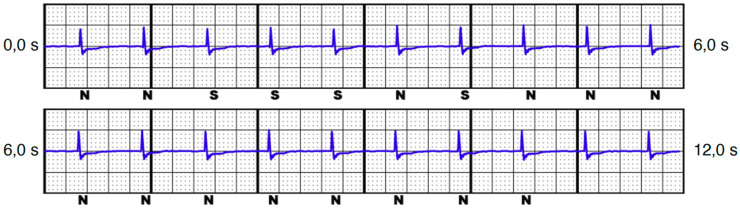
A total of 74 consecutive patients with a bipolar pacemaker were prospectively enrolled. First, surface rhythm strips were recorded in all possible pacemaker stimulation modes, to screen for T-wave oversensing (TWOS). Second, a S-ICD functional dummy was placed epicutaneously on the patient in the typical implant position. The same standardized pacing protocol was used as mentioned above, and every stimulation mode was recorded via S-ECG in all vectors.
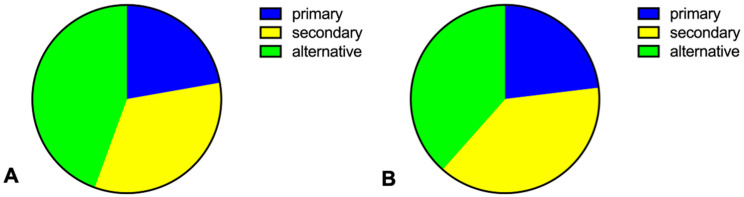
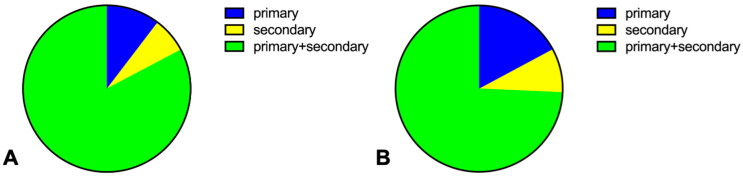
In 16 patients (21.6%), programmed stimulation would have led to VT/VF detection. Triggered episodes were due to counting of the pacing spike(s), QRS complex, premature ventricular contractions, and/or additional TWOS. Three cases triggered in the bipolar stimulation mode. Oversensing was associated with lung emphysema and a reduced QRS amplitude in the S-ECG.
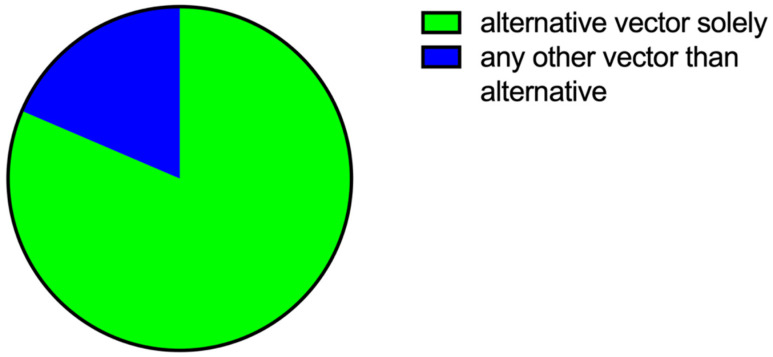
The combination of an S-ICD and a pacemaker may lead to inadequate shock delivery due to oversensing, even under programmed bipolar stimulation. Oversensing cannot be sufficiently predicted by the screening tool in pacemaker patients. Testing with an epicutaneous S-ICD dummy in all vectors and stimulation settings is recommended in patients with pre-existing pacemakers.
皮下植入式心律转复除颤器(S-ICD)的应用因无法提供备用起搏功能而受到限制。在某些情况下,将S-ICD与起搏器联合使用可能是一个不错的选择,但目前关于两者兼容性的经验有限。本研究的目的是确定S-ICD在起搏器患者中的安全性和有效性。
前瞻性纳入74例连续的双腔起搏器患者。首先,在所有可能的起搏器刺激模式下记录体表心电图节律条,以筛查T波感知过度(TWOS)。其次,将S-ICD功能性模拟装置经皮放置在患者的典型植入位置。使用与上述相同的标准化起搏方案,并通过体表心电图在所有向量中记录每种刺激模式。
16例患者(21.6%)中,程控刺激会导致室性心动过速/心室颤动检测。触发事件是由于起搏脉冲、QRS波群、室性早搏和/或额外的T波感知过度计数所致。3例在双极刺激模式下触发。感知过度与肺气肿和体表心电图中QRS波幅降低有关。
即使在程控双极刺激下,S-ICD与起搏器联合使用也可能因感知过度而导致电击发放不足。起搏器患者的筛查工具无法充分预测感知过度。对于已有起搏器的患者,建议在所有向量和刺激设置下使用经皮S-ICD模拟装置进行测试。