Bakkaloğlu Sevcan A, Özdemir Atikel Yeşim, Schmitt Claus Peter, Lévai Eszter, Adalat Shazia, Goodman Nadine, Dursun İsmail, Pınarbaşı Ayşe Seda, Yazıcıoğlu Burcu, Paglialonga Fabio, Vondrak Karel, Guzzo Isabella, Printza Nikoleta, Zurowska Aleksandra, Zagożdżon Ilona, Karabay Bayazıt Aysun, Atmış Bahriye, Tkaczyk Marcin, Faria Maria do Sameiro, Zaloszyc Ariane, Jankauskienė Augustina, Ekim Mesiha, Edefonti Alberto, Shroff Rukshana
Department of Pediatric Nephrology, Gazi University Faculty of Medicine, Ankara, Turkey.
Department of Pediatric Nephrology, Eskişehir City Hospital, Eskişehir, Turkey.
Clin Kidney J. 2023 Dec 28;17(1):sfad291. doi: 10.1093/ckj/sfad291. eCollection 2024 Jan.
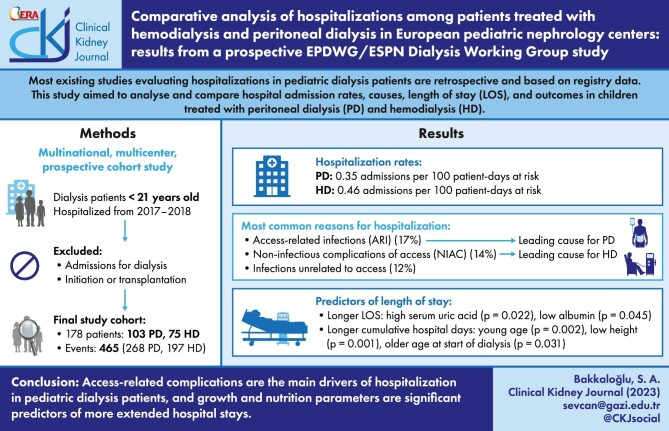
Hospital admissions in pediatric dialysis patients need to be better studied, and most existing studies are retrospective and based on registry data. This study aimed to analyse and compare hospital admission rates, causes, length of stay (LOS), and outcomes in children treated with peritoneal dialysis (PD) and hemodialysis (HD).
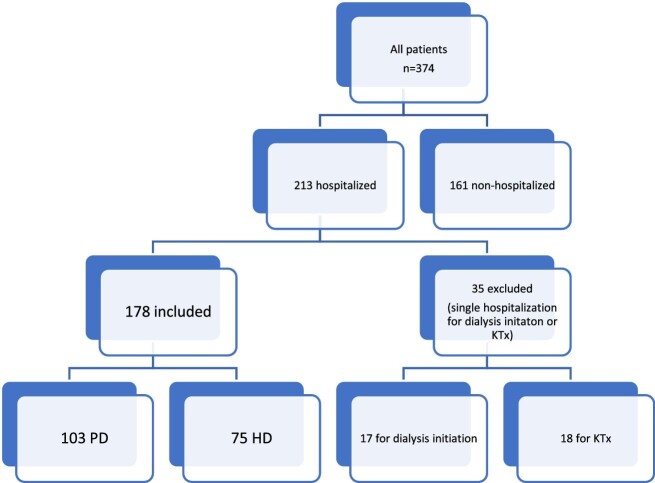
Data from 236 maintenance PD and 138 HD patients across 16 European dialysis centers were collected between 1 July 2017 and 30 June 2018. A total of 178 hospitalized patients (103 PD, 75 HD) were included for further analyses.
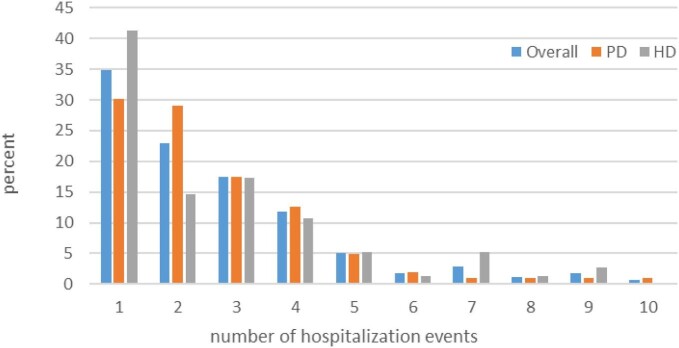
There were 465 hospitalization events (268 PD, 197 HD) with a rate of 0.39 admissions per 100 patient-days at risk (PDAR) and 2.4 hospital days per 100 PDAR. The admission rates were not significantly different between HD and PD patients. The most common causes of hospitalization were access-related infections (ARI) (17%), non-infectious complications of access (NIAC) (14%), and infections unrelated to access (12%). ARI was the leading cause in PD patients (24%), while NIAC was more common in HD patients (19%). PD patients had more ARIs, diagnostic procedures, and treatment adjustments (< .05), while HD patients had more NIACs, infections unrelated to access, access placement procedures, and interventional/surgical procedures (< .001). LOS was longer with acute admissions than non-acute admissions (< .001). Overall LOS and LOS in the intensive care unit were similar between HD and PD patients. High serum uric acid and low albumin levels were significant predictors of longer LOS (= .022 and = .045, respectively). Young age, more significant height deficit, and older age at the start of dialysis were predictors of longer cumulative hospital days (= .002, = .001, and = .031, respectively).
Access-related complications are the main drivers of hospitalization in pediatric dialysis patients, and growth and nutrition parameters are significant predictors of more extended hospital stays.
儿童透析患者的住院情况需要更深入研究,现有大多数研究为回顾性研究且基于登记数据。本研究旨在分析和比较接受腹膜透析(PD)和血液透析(HD)治疗的儿童的住院率、病因、住院时间(LOS)及预后。
收集了2017年7月1日至2018年6月30日期间16个欧洲透析中心236例维持性PD患者和138例HD患者的数据。共纳入178例住院患者(103例PD患者,75例HD患者)进行进一步分析。
共发生465次住院事件(268次PD,197次HD),每100患者日风险住院率(PDAR)为0.39次,每100 PDAR的住院天数为2.4天。HD患者和PD患者的住院率无显著差异。住院最常见的原因是与通路相关的感染(ARI)(17%)、通路的非感染性并发症(NIAC)(14%)以及与通路无关的感染(12%)。ARI是PD患者的主要住院原因(24%),而NIAC在HD患者中更常见(19%)。PD患者发生更多的ARI、诊断性操作和治疗调整(<0.05),而HD患者发生更多的NIAC、与通路无关的感染、通路置入操作以及介入/外科手术(<0.001)。急性入院的LOS比非急性入院更长(<0.001)。HD患者和PD患者的总体LOS以及在重症监护病房的LOS相似。高血清尿酸和低白蛋白水平是LOS延长的显著预测因素(分别为P = 0.022和P = 0.045)。年龄小、身高缺陷更明显以及透析开始时年龄较大是累计住院天数延长的预测因素(分别为P = 0.002、P = 0.001和P = 0.031)。
与通路相关的并发症是儿童透析患者住院的主要驱动因素,生长和营养参数是住院时间延长的显著预测因素。