University Hospital RWTH Aachen, Department of Pediatric Hematology, Oncology, and Stem Cell Transplantation, Aachen, Germany.
EBMT Paris Office, Hôpital Saint Antoine, Paris, France.
Bone Marrow Transplant. 2024 May;59(5):604-614. doi: 10.1038/s41409-024-02226-1. Epub 2024 Feb 8.
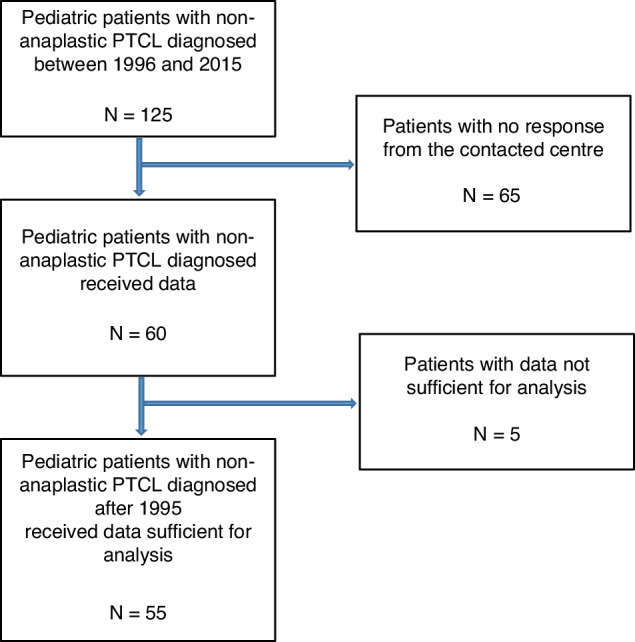
Peripheral T-cell lymphomas (PTCL) other than anaplastic large-cell lymphoma are rare in children, and the role of hematopoietic stem cell transplantation (HSCT) has not been clarified yet. In a retrospective analysis of registry-data of the European Society for Blood and Marrow Transplantation we analyzed 55 patients aged < 18 years who received allogeneic (N = 46) or autologous (N = 9) HSCT for PTCL. Median age at HSCT was 13.9 years; 33 patients (60%) were in first remission, and 6 (19%) in progression at HSCT. Conditioning was myeloablative in 87% of the allogeneic HSCTs and in 27 (58.7%) based on total body irradiation. After allogeneic HSCT the 5-year overall- and progression-free survival was 58.9% (95% CI 42.7-71.9) and 52.6% (95% CI 36.8-66.1), respectively. 5-year relapse incidence was 27.6% (95% CI 15.1-41.6), the non-relapse mortality rate was 19.8% (95% CI 9.7-32.6). Five of the six patients with progression at HSCT died. Seven of nine patients after autologous HSCT were alive and disease-free at last follow-up. Our data suggest a role of allogeneic HSCT in consolidation-treatment of patients with high-risk disease, who reach at least partial remission after primary- or relapse-therapy, whereas patients with therapy-refractory or progressive disease prior to transplantation do not profit from HSCT.
外周 T 细胞淋巴瘤(PTCL)除间变大细胞淋巴瘤外,在儿童中较为罕见,其造血干细胞移植(HSCT)的作用尚未明确。我们对欧洲血液和骨髓移植学会注册数据进行了回顾性分析,纳入了 55 名接受异基因(N=46)或自体(N=9)HSCT 治疗的 PTCL <18 岁的患者。HSCT 时的中位年龄为 13.9 岁;33 名患者(60%)处于首次缓解期,6 名(19%)在 HSCT 时处于进展期。87%的异基因 HSCT 采用清髓性预处理,27 例(58.7%)基于全身照射。异基因 HSCT 后 5 年总生存率和无进展生存率分别为 58.9%(95%CI 42.7-71.9)和 52.6%(95%CI 36.8-66.1)。5 年复发率为 27.6%(95%CI 15.1-41.6),非复发死亡率为 19.8%(95%CI 9.7-32.6)。6 名进展期患者中有 5 名死亡。9 名接受自体 HSCT 患者中有 7 名在最后一次随访时存活且无疾病。我们的数据表明,异基因 HSCT 可用于巩固治疗高危疾病患者,这些患者在初次或复发治疗后至少达到部分缓解,而移植前对治疗有抵抗或进展的患者不能从 HSCT 中获益。