Department of Neurology, GHU Paris Psychiatrie et Neurosciences Hôpital Sainte-Anne, Université Paris Cité, INSERM U1266, and FHU Neurovasc Paris France.
Department of Cardiology Hôpital Cochin, AP-HP, Université Paris Cité Paris France.
J Am Heart Assoc. 2024 Feb 20;13(4):e031684. doi: 10.1161/JAHA.123.031684. Epub 2024 Feb 14.
Patent foramen ovale (PFO) is causally associated with stroke in some patients younger than 60 years, especially when it is large or associated with an atrial septal aneurysm (ASA). After 60 years of age, this association is less well understood. We assessed the relationships between detailed atrial septal anatomy and the cryptogenic nature of stroke in this population.
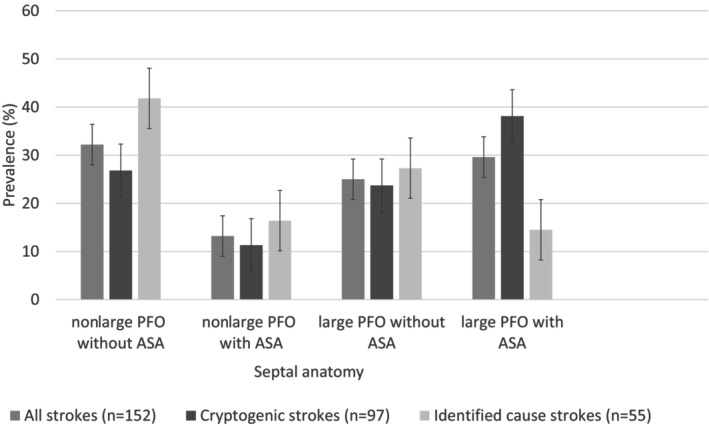
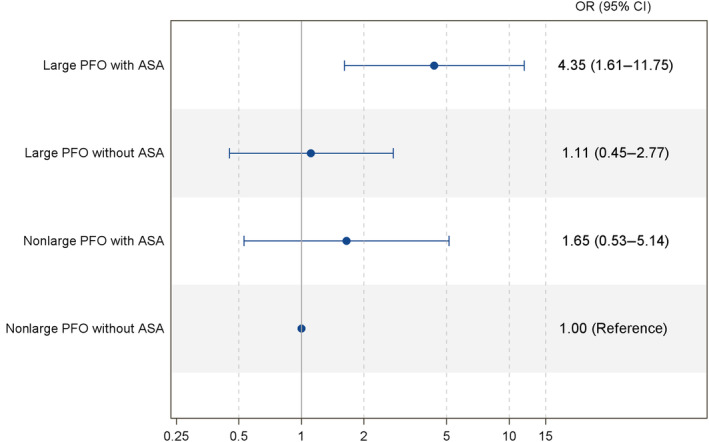
We reviewed all patients aged 60 to 80 years admitted to our stroke center for ischemic stroke who underwent contrast echocardiography between 2016 and 2021. The atherosclerosis, small-vessel disease, cardiac pathology, other causes, and dissection (ASCOD) classification was used to reevaluate the etiological workup. Associations between cryptogenic stroke and (1) PFO presence or (2) categories of PFO anatomy (nonlarge PFO without ASA, nonlarge PFO with ASA, large PFO without ASA, and large PFO with ASA) were assessed using logistic regression. Among 533 patients (median National Institutes of Health Stroke Scale score=1), PFO was present in 152 (prevalence, 28.5% [95% CI, 24.9-32.5]). Compared with noncryptogenic stroke, cryptogenic stroke (n=218) was associated with PFO presence (44.5% versus 17.5%; <0.0001). Among patients with a PFO, septal anatomy categories were associated with cryptogenic stroke (=0.02), with a strong association for patients with both large PFO and ASA (38.1% versus 14.5%, =0.002).
PFO presence remains strongly associated with cryptogenic stroke between 60 and 80 years of age. Large PFO, ASA, and their association were strongly associated with cryptogenic stroke in this age group. Our results support performing contrast echocardiography even after 60 years of age, although the optimal secondary prevention therapy in this population remains to be determined in randomized trials.
卵圆孔未闭(PFO)与一些 60 岁以下患者的中风有关,尤其是当 PFO 较大或伴有房间隔瘤(ASA)时。60 岁以后,这种关联就不太清楚了。我们评估了在这一年龄段人群中,详细的房间隔解剖结构与中风病因不明之间的关系。
我们回顾了 2016 年至 2021 年间在我们的中风中心因缺血性中风入院且接受对比超声心动图检查的所有 60 至 80 岁患者。采用动脉粥样硬化、小血管疾病、心脏病理学、其他原因和夹层(ASCOD)分类重新评估病因学检查。使用逻辑回归评估卵圆孔未闭(1)存在或(2)卵圆孔未闭解剖结构分类(无大卵圆孔未闭且无房间隔瘤、无大卵圆孔未闭且有房间隔瘤、大卵圆孔未闭且无房间隔瘤和大卵圆孔未闭且有房间隔瘤)与病因不明性中风之间的关联。在 533 例患者(中位数 NIHSS 评分为 1)中,有 152 例(152 例[95%CI:24.9-32.5])存在卵圆孔未闭。与非病因不明性中风相比,病因不明性中风(n=218)与卵圆孔未闭的存在相关(44.5%比 17.5%;<0.0001)。在存在卵圆孔未闭的患者中,隔瓣解剖结构类别与病因不明性中风相关(=0.02),大卵圆孔未闭和房间隔瘤并存与病因不明性中风的相关性最强(38.1%比 14.5%,=0.002)。
在 60 至 80 岁之间,卵圆孔未闭的存在与病因不明性中风仍有强烈关联。在该年龄组中,大卵圆孔未闭、房间隔瘤及其相关性与病因不明性中风密切相关。我们的结果支持即使在 60 岁以上也要进行对比超声心动图检查,尽管在随机试验中仍需要确定该人群的最佳二级预防治疗方法。