Doctoral Program in Medical Sciences, Faculty of Medicine, Universitas Indonesia, Jakarta, Indonesia; Department of Surgical Oncology, Dharmais Cancer Hospital-National Cancer Center, Jakarta, Indonesia.
Department of Plastic and Reconstructive Surgery, National Center for Global Health and Medicine, Tokyo, Japan.
J Vasc Surg Venous Lymphat Disord. 2024 Jul;12(4):101863. doi: 10.1016/j.jvsv.2024.101863. Epub 2024 Feb 28.
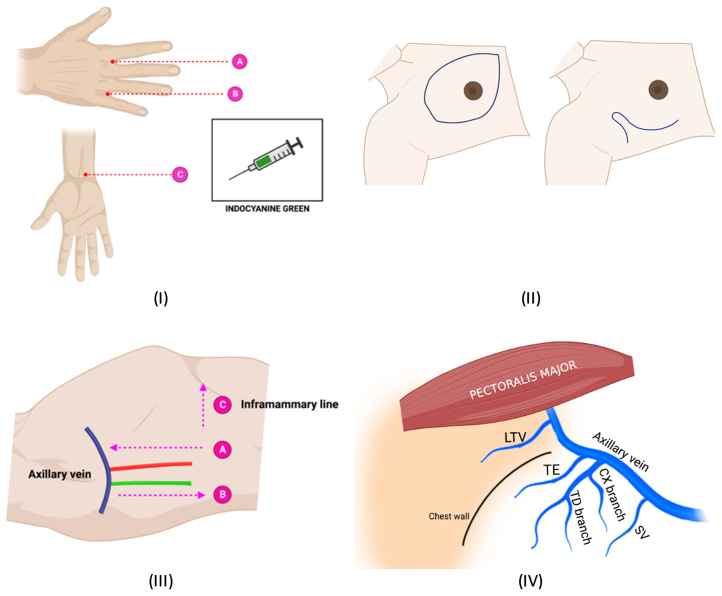
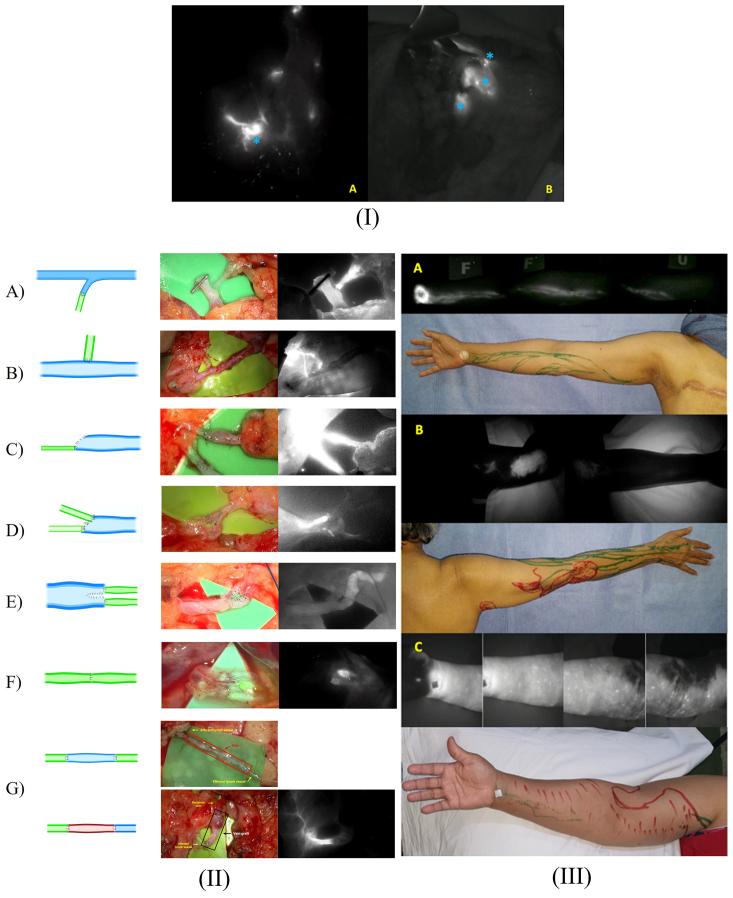
We describe the feasibility and short-term outcome of our surgical technique to repair the lymph vessel disruption directly after axillary lymph node dissection during breast cancer surgery. This procedure is called immediate lymphatic reconstruction to prevent breast cancer treatment-related lymphedema (BCRL), which frequently occurs after axillary lymph node dissection. The surgical technique consisted of lymphaticovenous anastomosis (LVA) or lymphaticolymphatic anastomosis. We named the procedure lymphatic bypass supermicrosurgery (LBS).
This study used a retrospective cohort design of patients with breast cancer between May 2020 and February 2023. LBS was performed by making an intima-to-intima coaptation between afferent lymph vessels and the recipient's veins (LVA) or efferent lymph vessels lymphaticolymphatic anastomosis.
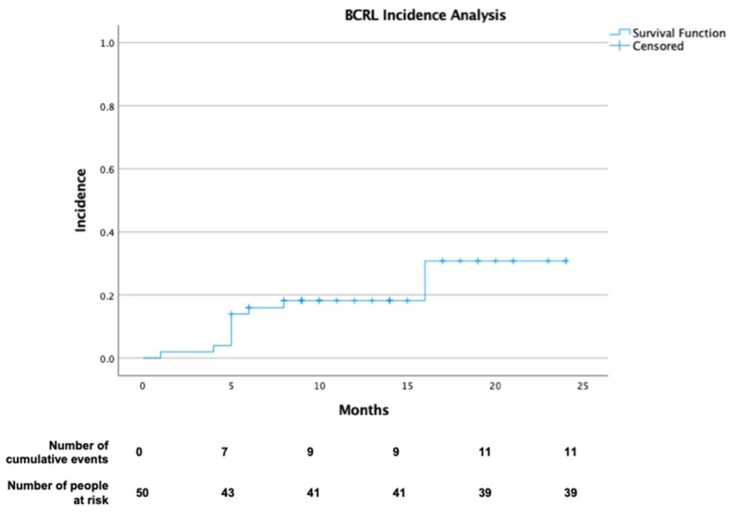
A total of 82 patients underwent lymphatic bypass. The mean age of patients was 50 ± 12 years, and most had stage III breast cancer (n = 59 [72%]). LVA was the most common type of lymphatic bypass (94.6%). The median number of LVA was 1 (range, 1-4) and 1 (range, 1-3) for lymphaticolymphatic anastomosis. The median follow-up time was 12.5 months (range, 1-33 months). The 50 patients who had postoperative indocyanine green lymphography described arm dermal backflow stage 0 in 20 (40%), stage 1 in 19 (38%), stage 2 in 2 (4%), and stage 3 in 9 (18%) cases. The proportion of BCRL was 11 (22%), and subclinical lymphedema was 19 (38%) in this period. Most cases were in stable subclinical lymphedema (10, 58.8%). The 1-year and 2-year BCRL rates were 14% (95% confidence interval, 4%-23.9%) and 22% (95% confidence interval, 10.1%-33.9%), respectively.
Along with the emerging immediate lymphatic reconstruction, LBS is a feasible supermicrosurgery technique that may have a potential role in BCRL prevention. A randomized controlled study would confirm the effectiveness of the technique.
我们描述了一种在乳腺癌手术中直接修复腋窝淋巴结清扫术后淋巴管破裂的手术技术的可行性和短期结果。该手术被称为即刻淋巴重建术,以预防乳腺癌治疗相关淋巴水肿(BCRL),这在腋窝淋巴结清扫术后很常见。手术技术包括淋巴管静脉吻合术(LVA)或淋巴管淋巴管吻合术。我们将该手术命名为淋巴旁路超微外科手术(LBS)。
本研究采用回顾性队列设计,纳入 2020 年 5 月至 2023 年 2 月期间的乳腺癌患者。LBS 通过在输入淋巴管和受体静脉(LVA)之间或输出淋巴管淋巴管吻合术之间进行内膜对内膜贴合来进行。
共有 82 名患者接受了淋巴旁路手术。患者的平均年龄为 50 ± 12 岁,大多数为 III 期乳腺癌(n=59 [72%])。LVA 是最常见的淋巴旁路类型(94.6%)。LVA 的中位数为 1 个(范围为 1-4 个),淋巴管淋巴管吻合术的中位数为 1 个(范围为 1-3 个)。中位随访时间为 12.5 个月(范围为 1-33 个月)。50 名接受术后吲哚菁绿淋巴管造影术的患者中,20 名(40%)手臂真皮回流处于 0 期,19 名(38%)处于 1 期,2 名(4%)处于 2 期,9 名(18%)处于 3 期。BCRL 的比例为 11 例(22%),在此期间亚临床淋巴水肿为 19 例(38%)。大多数患者处于稳定的亚临床淋巴水肿状态(10 例,58.8%)。1 年和 2 年的 BCRL 发生率分别为 14%(95%置信区间,4%-23.9%)和 22%(95%置信区间,10.1%-33.9%)。
随着即刻淋巴重建术的出现,LBS 是一种可行的超微外科技术,可能在预防 BCRL 方面发挥作用。一项随机对照研究将证实该技术的有效性。