Division of Nephrology, Department of Medicine, University of Texas Health San Antonio, San Antonio, Texas, USA
Nephrology Division, Federal University of São Paulo, São Paulo, Brazil.
BMJ Open. 2024 Mar 19;14(3):e076444. doi: 10.1136/bmjopen-2023-076444.
This study aimed to evaluate the efficacy and safety of finerenone, a selective, non-steroidal mineralocorticoid receptor antagonist, on cardiovascular and kidney outcomes by age and/or sex.
FIDELITY post hoc analysis; median follow-up of 3 years.
FIDELITY: a prespecified analysis of the FIDELIO-DKD and FIGARO-DKD trials.
Adults with type 2 diabetes and chronic kidney disease receiving optimised renin-angiotensin system inhibitors (N=13 026).
Randomised 1:1; finerenone or placebo.
Cardiovascular (cardiovascular death, non-fatal myocardial infarction, non-fatal stroke or hospitalisation for heart failure (HHF)) and kidney (kidney failure, sustained ≥57% estimated glomerular filtration rate (eGFR) decline or renal death) composite outcomes.
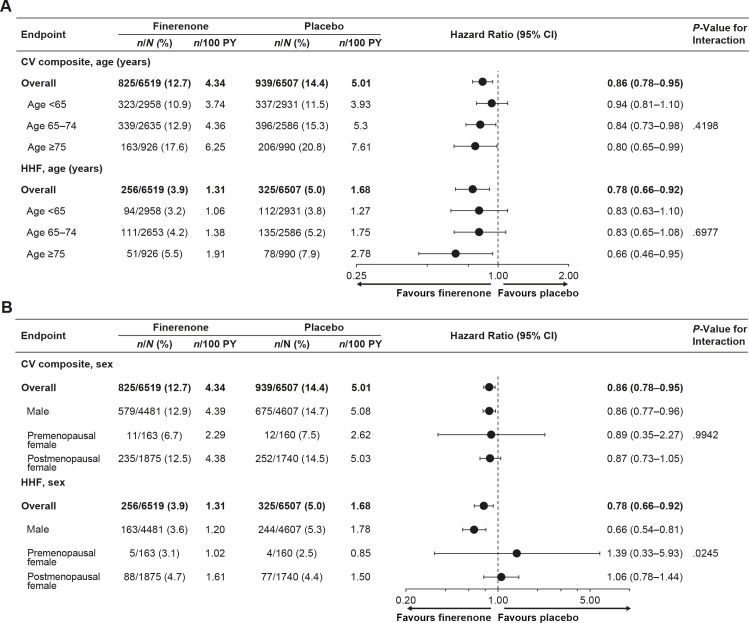
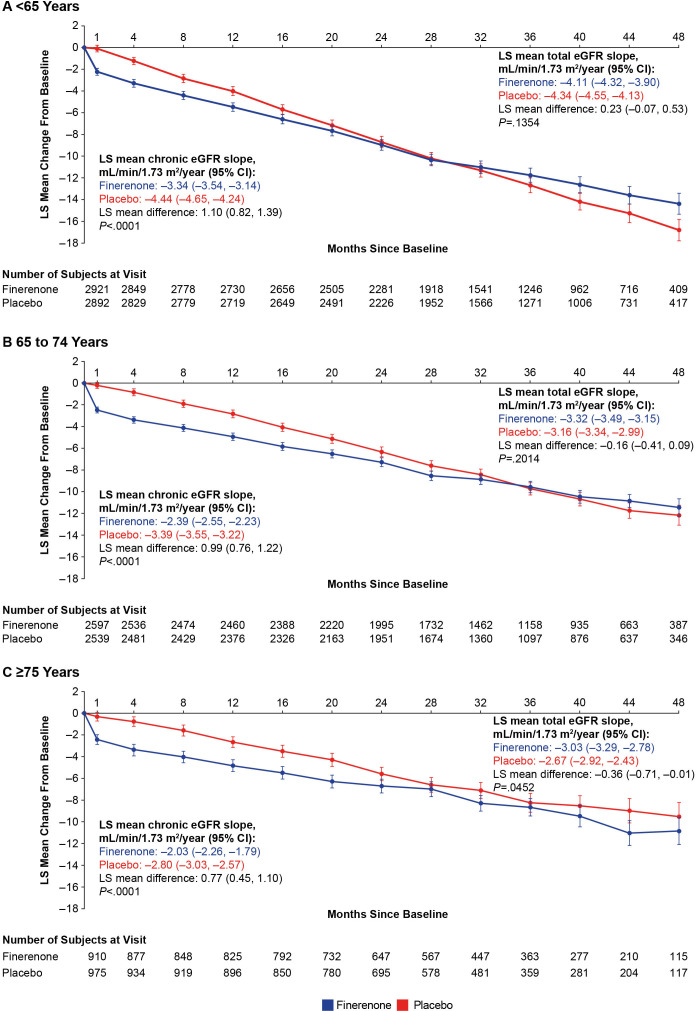
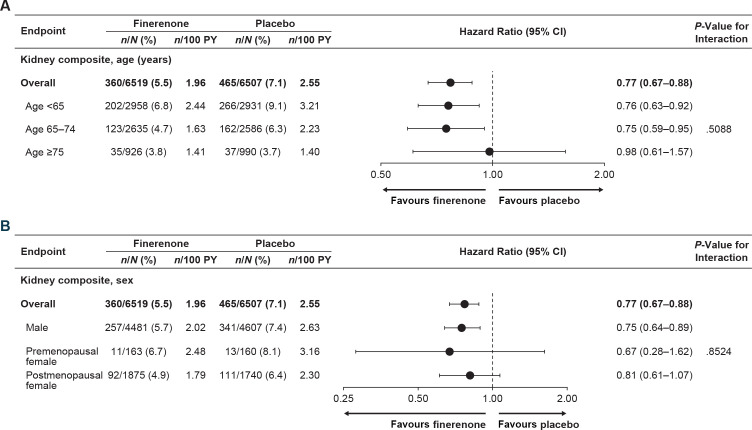
Mean age was 64.8 years; 45.2%, 40.1% and 14.7% were aged <65, 65-74 and ≥75 years, respectively; 69.8% were male. Cardiovascular benefits of finerenone versus placebo were consistent across age (HR 0.94 (95% CI 0.81 to 1.10) (<65 years), HR 0.84 (95% CI 0.73 to 0.98) (65-74 years), HR 0.80 (95% CI 0.65 to 0.99) (≥75 years); P=0.42) and sex categories (HR 0.86 (95% CI 0.77 to 0.96) (male), HR 0.89 (95% CI 0.35 to 2.27) (premenopausal female), HR 0.87 (95% CI 0.73 to 1.05) (postmenopausal female); P=0.99). Effects on HHF reduction were not modified by age (P=0.70) but appeared more pronounced in males (P=0.02). Kidney events were reduced with finerenone versus placebo in age groups <65 and 65-74 but not ≥75; no heterogeneity in treatment effect was observed (P=0.51). In sex subgroups, finerenone consistently reduced kidney events (P=0.85). Finerenone reduced albuminuria and eGFR decline regardless of age and sex. Hyperkalaemia increased with finerenone, but discontinuation rates were <3% across subgroups. Gynaecomastia in males was uncommon across age subgroups and identical between treatment groups.
Finerenone improved cardiovascular and kidney composite outcomes with no significant heterogeneity between age and sex subgroups; however, the effect on HHF appeared more pronounced in males. Finerenone demonstrated a similar safety profile across age and sex subgroups.
NCT02540993, NCT02545049.
本研究旨在评估选择性非甾体类盐皮质激素受体拮抗剂非奈利酮在心血管和肾脏结局方面的疗效和安全性,分别按年龄和/或性别进行评估。
FIDELITY 事后分析;中位随访 3 年。
FIDELITY:FIDELIO-DKD 和 FIGARO-DKD 试验的预设分析。
接受优化的肾素-血管紧张素系统抑制剂治疗的 2 型糖尿病和慢性肾脏病成人(N=13026)。
随机 1:1;非奈利酮或安慰剂。
心血管(心血管死亡、非致死性心肌梗死、非致死性卒中和因心力衰竭住院(HHF))和肾脏(肾衰竭、持续≥57%估计肾小球滤过率(eGFR)下降或肾脏死亡)复合结局。
平均年龄为 64.8 岁;<65 岁、65-74 岁和≥75 岁的比例分别为 45.2%、40.1%和 14.7%;69.8%为男性。非奈利酮与安慰剂相比,在心血管方面的获益在年龄组之间是一致的(HR 0.94(95%CI 0.81 至 1.10)(<65 岁),HR 0.84(95%CI 0.73 至 0.98)(65-74 岁),HR 0.80(95%CI 0.65 至 0.99)(≥75 岁);P=0.42)和性别类别(HR 0.86(95%CI 0.77 至 0.96)(男性),HR 0.89(95%CI 0.35 至 2.27)(绝经前女性),HR 0.87(95%CI 0.73 至 1.05)(绝经后女性);P=0.99)。在年龄方面,非奈利酮对 HHF 减少的影响没有差异(P=0.70),但在男性中更为明显(P=0.02)。与安慰剂相比,非奈利酮降低了年龄<65 岁和 65-74 岁的肾脏事件,但不能降低≥75 岁的肾脏事件;治疗效果没有异质性(P=0.51)。在性别亚组中,非奈利酮一致降低了肾脏事件(P=0.85)。非奈利酮无论年龄和性别如何均可降低蛋白尿和 eGFR 下降。非奈利酮可增加高钾血症,但各亚组的停药率均<3%。男性的乳腺发育在各年龄组中都不常见,并且在治疗组之间是相同的。
非奈利酮改善了心血管和肾脏复合结局,在年龄和性别亚组之间没有显著的异质性;然而,非奈利酮在男性中的 HHF 效果似乎更为明显。非奈利酮在各年龄和性别亚组中具有相似的安全性特征。
NCT02540993,NCT02545049。