Michelson Andrew P, Lyons Patrick G, Nguyen Nguyet M, Reynolds Daniel, McDonald Rachel, McEvoy Colleen A, Despotovic Vladimir, Brody Steven L, Kollef Marin H, Kraft Bryan D
Division of Pulmonary and Critical Care Medicine, Washington University School of Medicine, Saint Louis, MO.; Department of Medicine, the Institute for Informatics, Washington University School of Medicine, Saint Louis, MO.
Division of Pulmonary and Critical Care Medicine, Washington University School of Medicine, Saint Louis, MO.
CHEST Crit Care. 2023 Dec;1(3). doi: 10.1016/j.chstcc.2023.100019. Epub 2023 Sep 25.
The clinical benefit of using inhaled epoprostenol (iEpo) through a humidified high-flow nasal cannula (HHFNC) remains unknown for patients with COVID-19.
Can iEpo prevent respiratory deterioration for patients with positive SARS-CoV-2 findings receiving HHFNC?
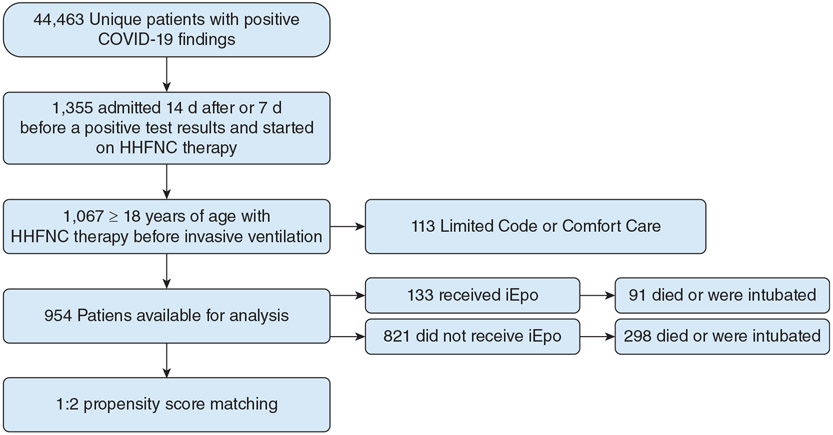
This multicenter retrospective cohort analysis included patients aged 18 years or older with COVID-19 pneumonia who required HHFNC treatment. Patients who received iEpo were propensity score matched to patients who did not receive iEpo. The primary outcome was time to mechanical ventilation or death without mechanical ventilation and was assessed using Kaplan-Meier curves and Cox proportional hazard ratios. The effects of residual confounding were assessed using a multilevel analysis, and a secondary analysis adjusted for outcome propensity also was performed in a multivariable model that included the entire (unmatched) patient cohort.
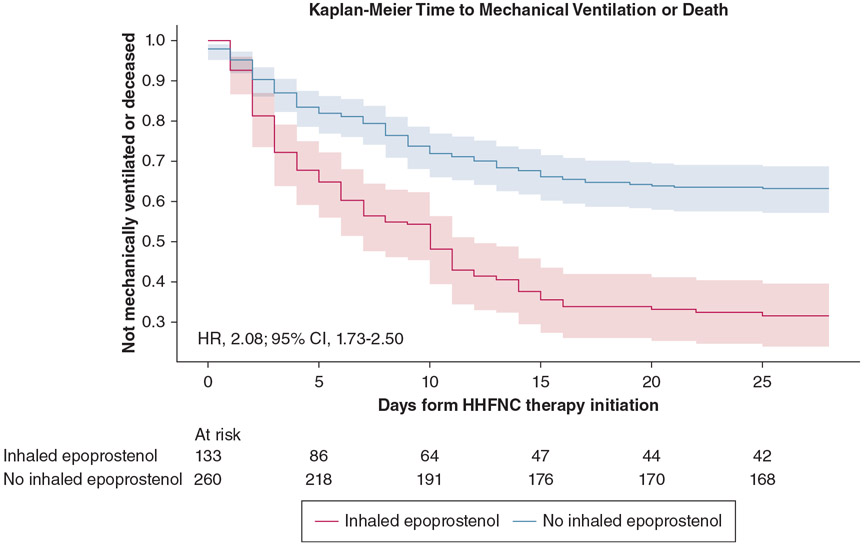
Among 954 patients with positive SARS-CoV-2 findings receiving HHFNC therapy, 133 patients (13.9%) received iEpo. After propensity score matching, the median number of days until the composite outcome was similar between treatment groups (iEpo: 5.0 days [interquartile range, 2.0-10.0 days] vs no-iEpo: 6.5 days [interquartile range, 2.0-11.0 days]; = .26), but patients who received iEpo were more likely to meet the composite outcome in the propensity score-matched, multilevel, and multivariable unmatched analyses (hazard ratio, 2.08 [95% CI, 1.73-2.50]; OR, 4.72 [95% CI, 3.01-7.41]; and OR, 1.35 [95% CI, 1.23-1.49]; respectively).
In patients with COVID-19 receiving HHFNC therapy, use of iEpo was associated with the need for invasive mechanical ventilation.
对于新型冠状病毒肺炎(COVID-19)患者,通过湿热高流量鼻导管(HHFNC)使用吸入性依前列醇(iEpo)的临床益处尚不清楚。
对于严重急性呼吸综合征冠状病毒2(SARS-CoV-2)检测呈阳性且接受HHFNC治疗的患者,iEpo能否预防呼吸功能恶化?
这项多中心回顾性队列分析纳入了年龄在18岁及以上、患有COVID-19肺炎且需要HHFNC治疗的患者。接受iEpo治疗的患者与未接受iEpo治疗的患者进行倾向评分匹配。主要结局是开始机械通气的时间或未进行机械通气的死亡时间,并使用Kaplan-Meier曲线和Cox比例风险比进行评估。使用多水平分析评估残余混杂因素的影响,并在包含整个(未匹配)患者队列的多变量模型中对结局倾向进行调整后进行二次分析。
在954例接受HHFNC治疗且SARS-CoV-2检测呈阳性的患者中,133例(13.9%)接受了iEpo治疗。倾向评分匹配后,各治疗组直至复合结局的中位天数相似(iEpo组:5.0天[四分位间距,2.0 - 10.0天],未使用iEpo组:6.5天[四分位间距,2.0 - 11.0天];P = 0.26),但在倾向评分匹配、多水平和多变量未匹配分析中,接受iEpo治疗的患者更有可能达到复合结局(风险比,2.08[95%置信区间,1.73 - 2.50];比值比,4.72[95%置信区间,3.01 - 7.41];以及比值比,1.35[95%置信区间,1.23 - 1.49])。
在接受HHFNC治疗的COVID-19患者中,使用iEpo与有创机械通气的需求相关。