Göbel Nora, Holder Simone, Hüther Franziska, Anguelov Yasemin, Bail Dorothee, Franke Ulrich
Department of Cardiovascular Surgery, Robert-Bosch-Hospital, Stuttgart, Germany.
Front Cardiovasc Med. 2024 Mar 15;11:1326124. doi: 10.3389/fcvm.2024.1326124. eCollection 2024.
The extent of surgery and the role of the frozen elephant trunk (FET) for surgical repair of acute aortic dissection type I are still subjects of debate. The aim of the study is to evaluate the short- and long-term results of acute surgical repair of aortic dissection type I using the FET compared to standard proximal aortic repair.
Between October 2009 and December 2016, 172 patients underwent emergent surgery for acute type I aortic dissection at our center. Of these, = 72 received a FET procedure, while the other 100 patients received a conventional proximal aortic repair. Results were compared between the two surgery groups. The primary endpoints included 30-day rates of mortality and neurologic deficit and follow-up rates of mortality and aortic-related reintervention.
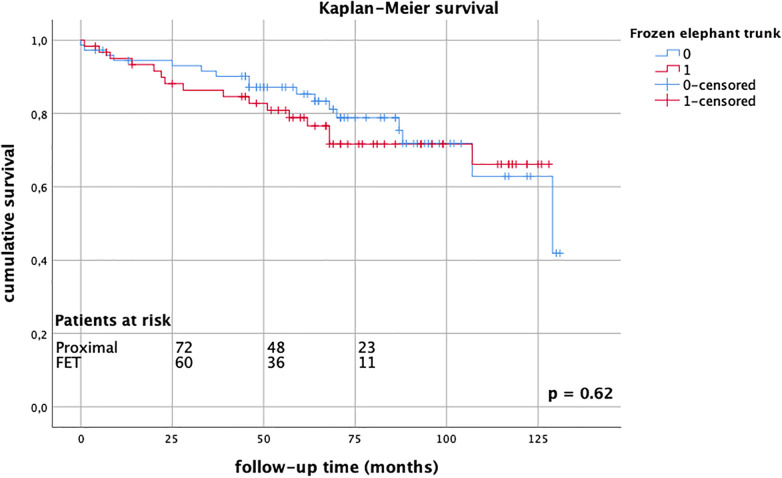
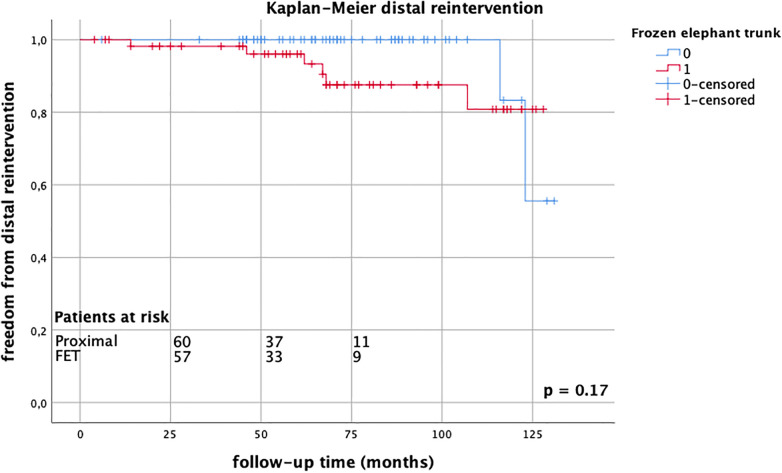
Demographic data were comparable between the groups, except for a higher proportion of men in the FET group (76.4% vs. 60.0%, = 0.03). The median age was 62 years [IQR (20), = 0.17], and the median log EuroSCORE was 38.6% [IQR (31.4), = 0.21]. The mean follow-up time was 68.3 ± 33.8 months. Neither early (FET group 15.3% vs. proximal group 23.0%, = 0.25) nor late (FET group 26.2% vs. proximal group 23.0%, = 0.69) mortality showed significant differences between the groups. There were fewer strokes in the FET patients (FET group 2.8% vs. proximal group 11.0%, = 0.04), and the rates of spinal cord injury were similar between the groups (FET group 4.2% vs. proximal group 2.0%, = 0.41). Aortic-related reintervention rates did not differ between the groups (FET group 12.1% vs. proximal group 9.8%, = 0.77).
Emergent FET repair for acute aortic dissection type I is safe and feasible when performed by experienced surgeons. The benefits of the FET procedure in the long term remain unclear. Prolonged follow-up data are needed.
对于I型急性主动脉夹层的手术范围及冰冻象鼻术(FET)在手术修复中的作用仍存在争议。本研究的目的是评估与标准近端主动脉修复相比,使用FET进行I型主动脉夹层急性手术修复的短期和长期结果。
2009年10月至2016年12月期间,172例患者在本中心接受了I型急性主动脉夹层的急诊手术。其中,72例接受了FET手术,而其他100例患者接受了传统的近端主动脉修复。比较两组手术的结果。主要终点包括30天死亡率和神经功能缺损率以及死亡率和主动脉相关再次干预的随访率。
除FET组男性比例较高(76.4%对60.0%,P = 0.03)外,两组间人口统计学数据具有可比性。中位年龄为62岁[四分位间距(IQR)(20),P = 0.17],中位欧洲心脏手术风险评估系统(EuroSCORE)评分为38.6%[IQR(31.4),P = 0.21]。平均随访时间为68.3±33.8个月。两组间早期(FET组15.3%对近端组23.0%,P = 0.25)和晚期(FET组26.2%对近端组23.0%,P = 0.69)死亡率均无显著差异。FET患者中风较少(FET组2.8%对近端组11.0%,P = 0.04),两组脊髓损伤发生率相似(FET组4.2%对近端组2.0%,P = 0.41)。两组间主动脉相关再次干预率无差异(FET组12.1%对近端组9.8%,P = 0.77)。
由经验丰富的外科医生进行I型急性主动脉夹层的急诊FET修复是安全可行的。FET手术的长期益处仍不清楚。需要长期随访数据。