Department of Endocrine Surgery, Kanagawa Cancer Center, Kanagawa 241-8515, Japan.
Department of Breast and Thyroid Surgery, Yokohama City University Medical Center, Kanagawa 232-0024, Japan.
J Clin Endocrinol Metab. 2024 Oct 15;109(11):2784-2792. doi: 10.1210/clinem/dgae271.
The relationship between the genomic profile and prognosis of advanced thyroid carcinoma requiring drug therapy has not been reported.
To evaluate the treatment period and overall survival time for each genetic alteration in advanced thyroid carcinoma that requires drug therapy.
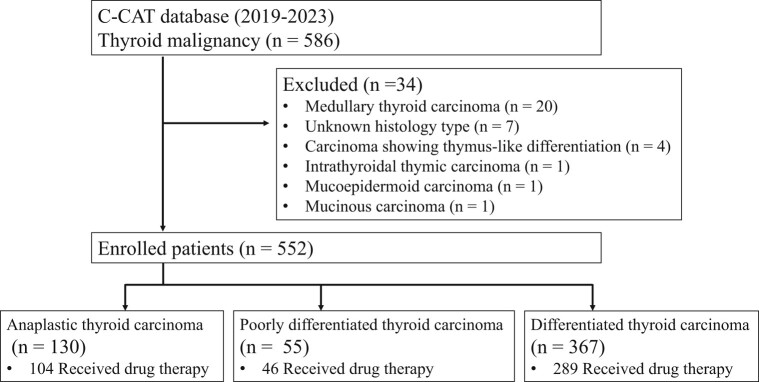
We conducted a retrospective observational study using a national database in Japan, which included 552 cases of thyroid carcinoma out of 53 543 patients in the database.
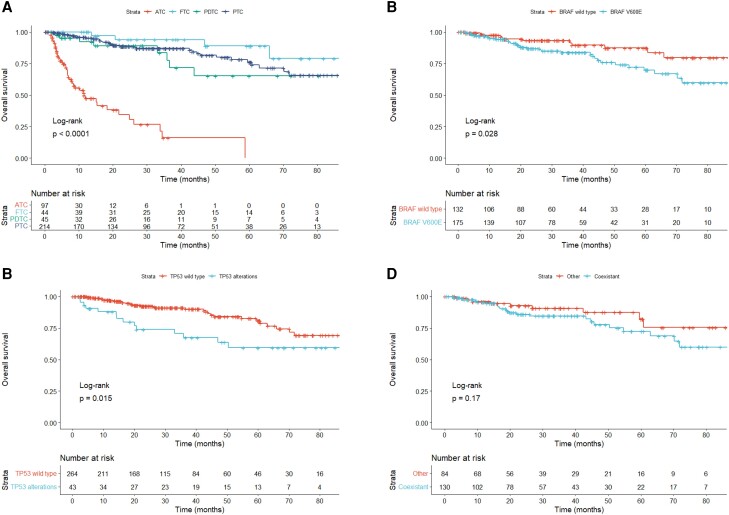
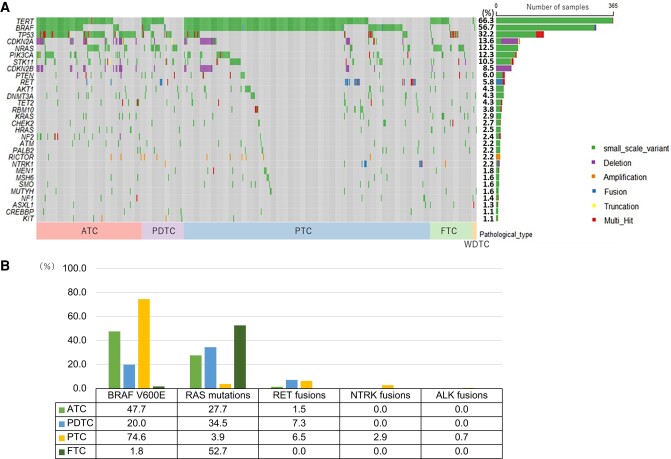
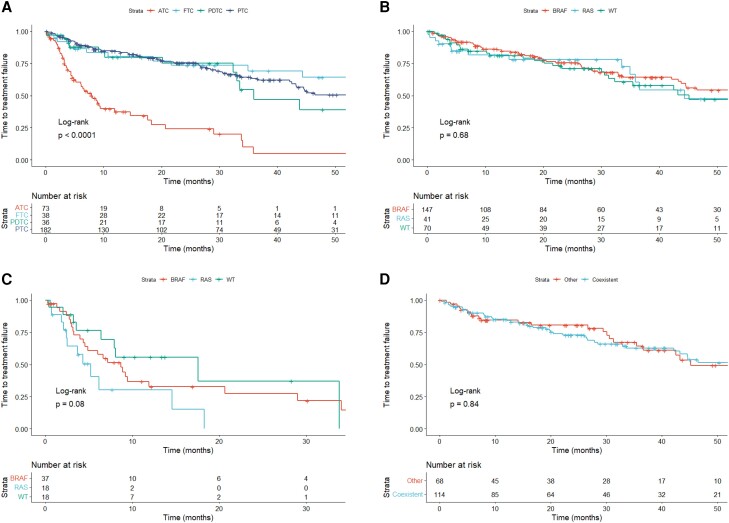
The database included anaplastic thyroid carcinoma (23.6%), poorly differentiated thyroid carcinoma (10.0%), and differentiated thyroid carcinoma (66.4%). The most common genetic abnormalities were TERT promoter (66.3%), BRAF (56.7%), and TP53 (32.2%). The typical driver genes were BRAF V600E (55.0%), RAS (18.5%), RET fusion (4.7%), NTRK fusion (1.6%), and ALK fusion (0.4%). The most common regimen was lenvatinib, and the time to treatment failure was not different despite the presence of BRAF or RAS mutations. In differentiated thyroid carcinoma and poorly differentiated thyroid carcinoma, TP53 alterations independently predicted worse overall survival (hazard ratio = 2.205, 95% confidence interval: 1.135-4.283). In anaplastic thyroid carcinoma, no genetic alterations were associated with overall survival.
Genetic abnormalities with treatment options were found in 62.7% of advanced thyroid carcinomas. TP53 abnormality was an independent poor prognostic factor for overall survival in differentiated thyroid carcinoma. The time to treatment failure for lenvatinib was not different based on genetic profile.
尚未有研究报道药物治疗的晚期甲状腺癌的基因组特征与预后之间的关系。
评估每种需要药物治疗的晚期甲状腺癌的基因改变的治疗持续时间和总生存时间。
我们使用日本的一个全国性数据库进行了回顾性观察性研究,该数据库包括 53543 例患者中的 552 例甲状腺癌病例。
该数据库包括间变性甲状腺癌(23.6%)、低分化甲状腺癌(10.0%)和分化型甲状腺癌(66.4%)。最常见的遗传异常是 TERT 启动子(66.3%)、BRAF(56.7%)和 TP53(32.2%)。典型的驱动基因是 BRAF V600E(55.0%)、RAS(18.5%)、RET 融合(4.7%)、NTRK 融合(1.6%)和 ALK 融合(0.4%)。最常见的方案是仑伐替尼,尽管存在 BRAF 或 RAS 突变,但治疗失败的时间没有差异。在分化型甲状腺癌和低分化甲状腺癌中,TP53 改变独立预测总生存不良(风险比=2.205,95%置信区间:1.135-4.283)。在间变性甲状腺癌中,没有遗传改变与总生存相关。
在 62.7%的晚期甲状腺癌中发现了具有治疗选择的遗传异常。TP53 异常是分化型甲状腺癌总生存的独立不良预后因素。仑伐替尼的治疗失败时间与基因谱无关。