Department of Medicine, University of Toledo College of Medicine and Life Sciences, Toledo, Ohio, United States.
Department of Pathology, Lipidomics Core Facility, Wayne State University, Detroit, Michigan, United States.
Am J Physiol Heart Circ Physiol. 2024 Jun 1;326(6):H1498-H1514. doi: 10.1152/ajpheart.00068.2024. Epub 2024 Apr 19.
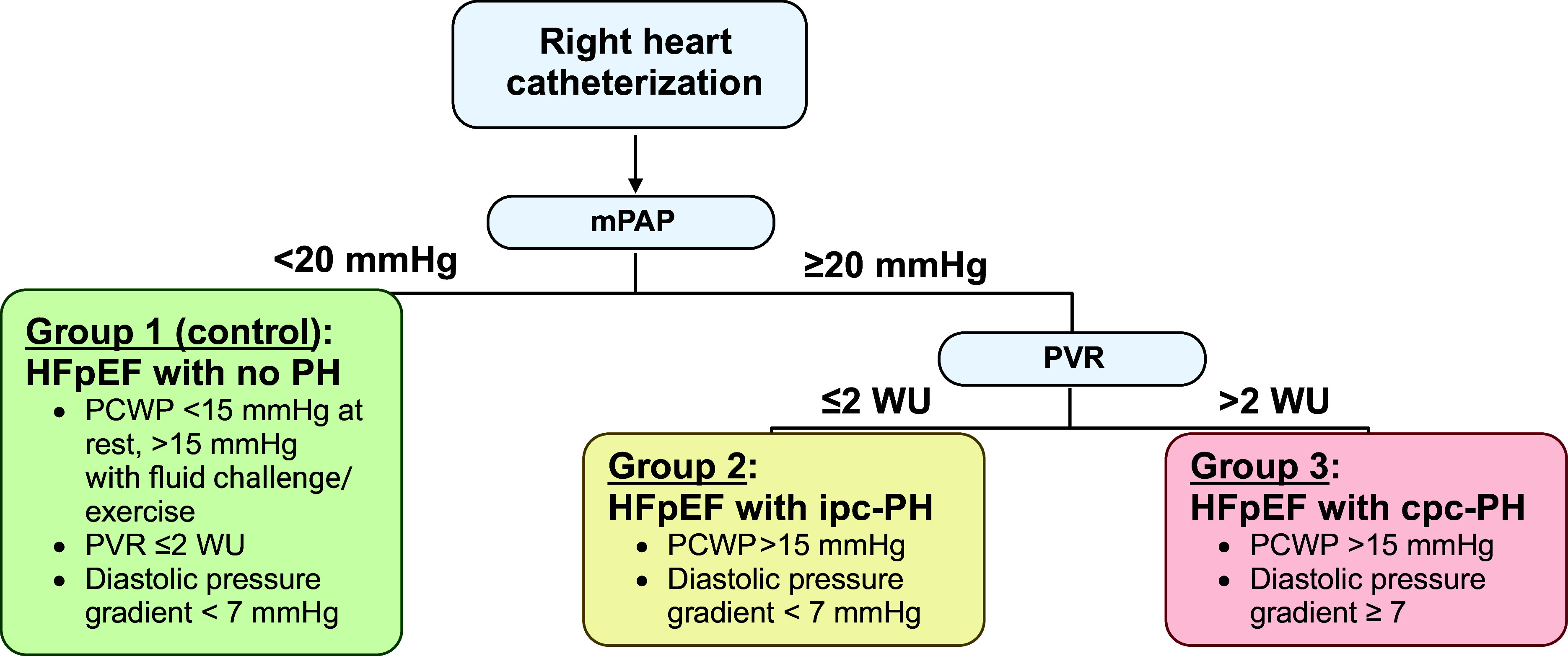
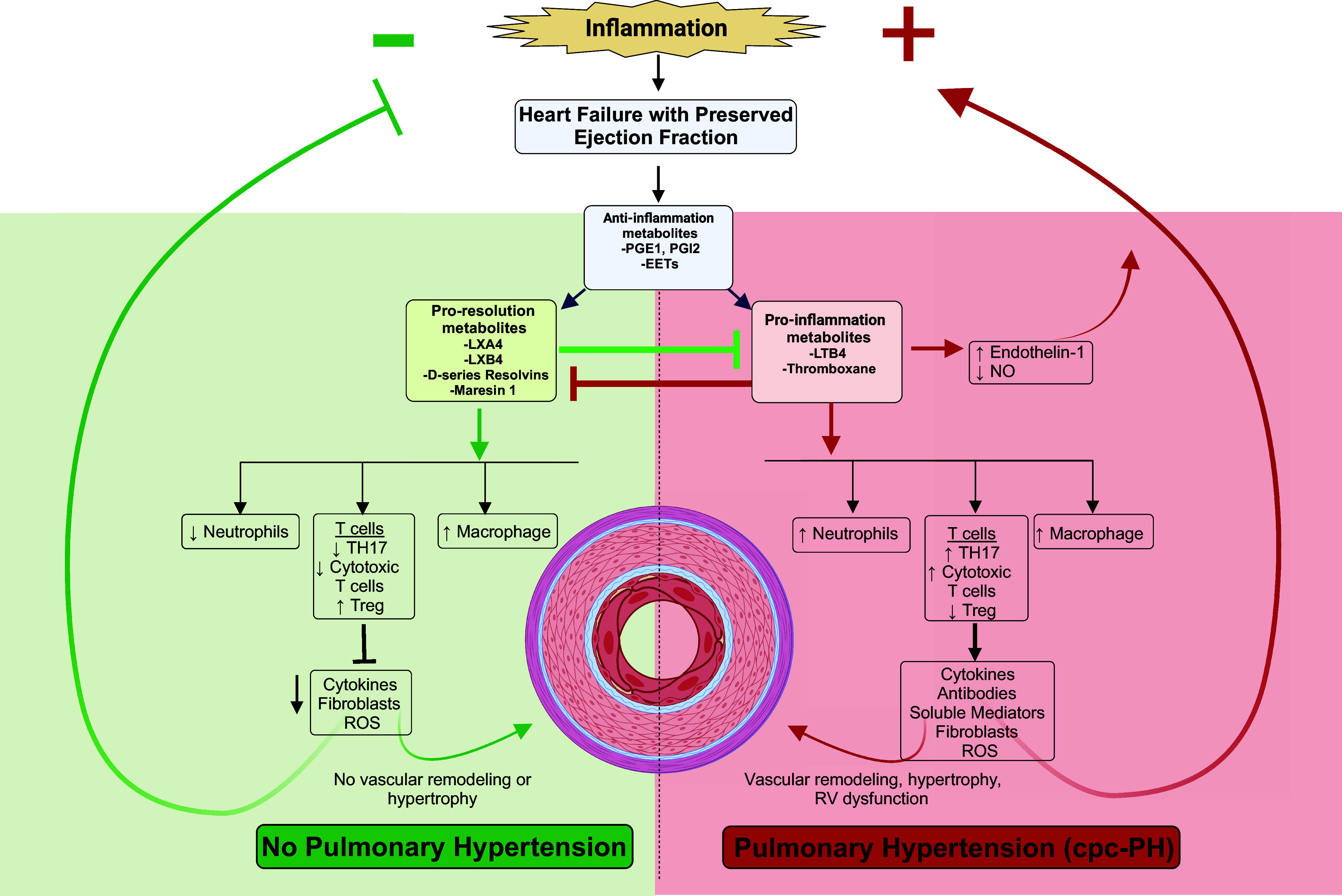
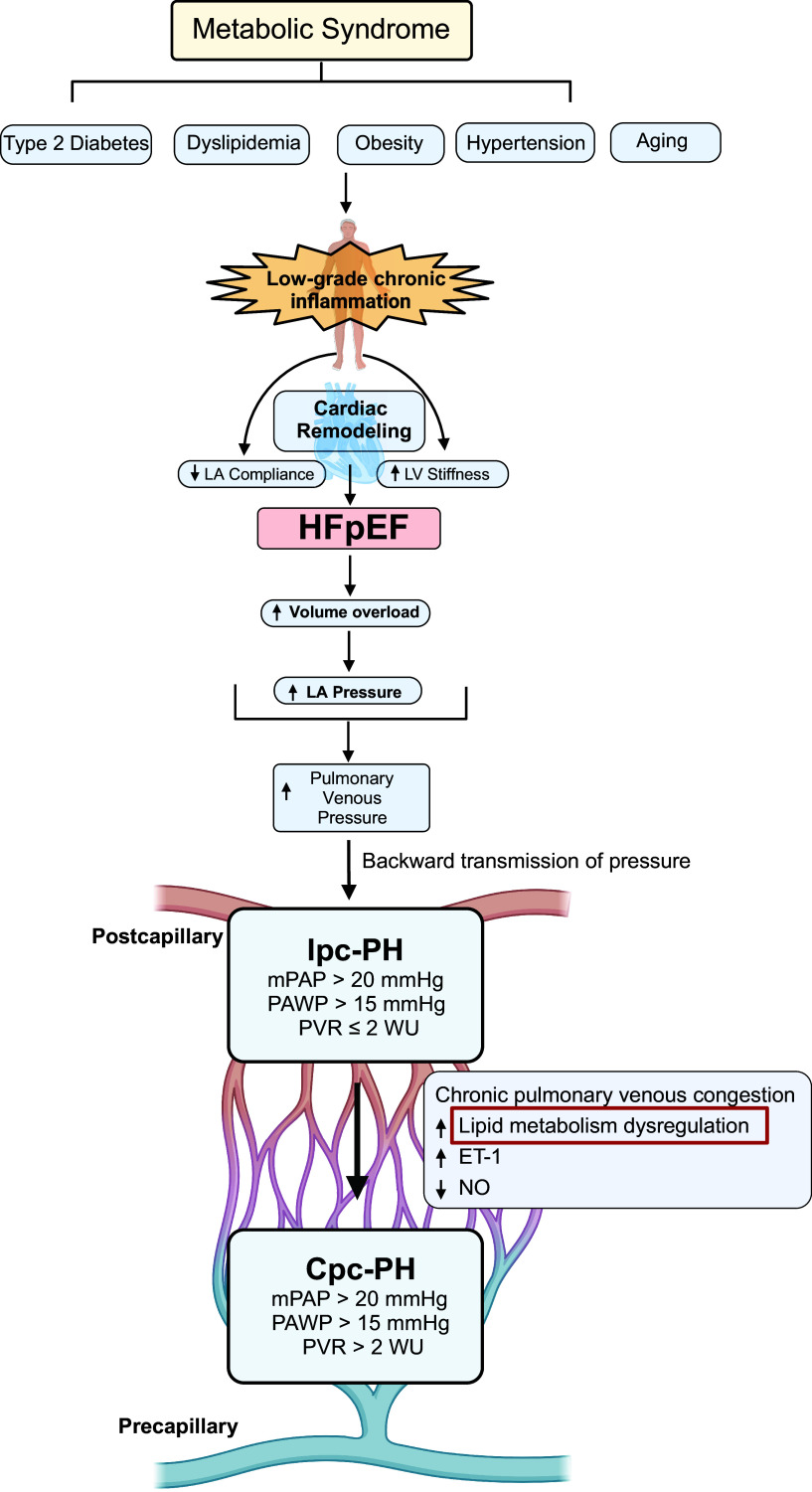
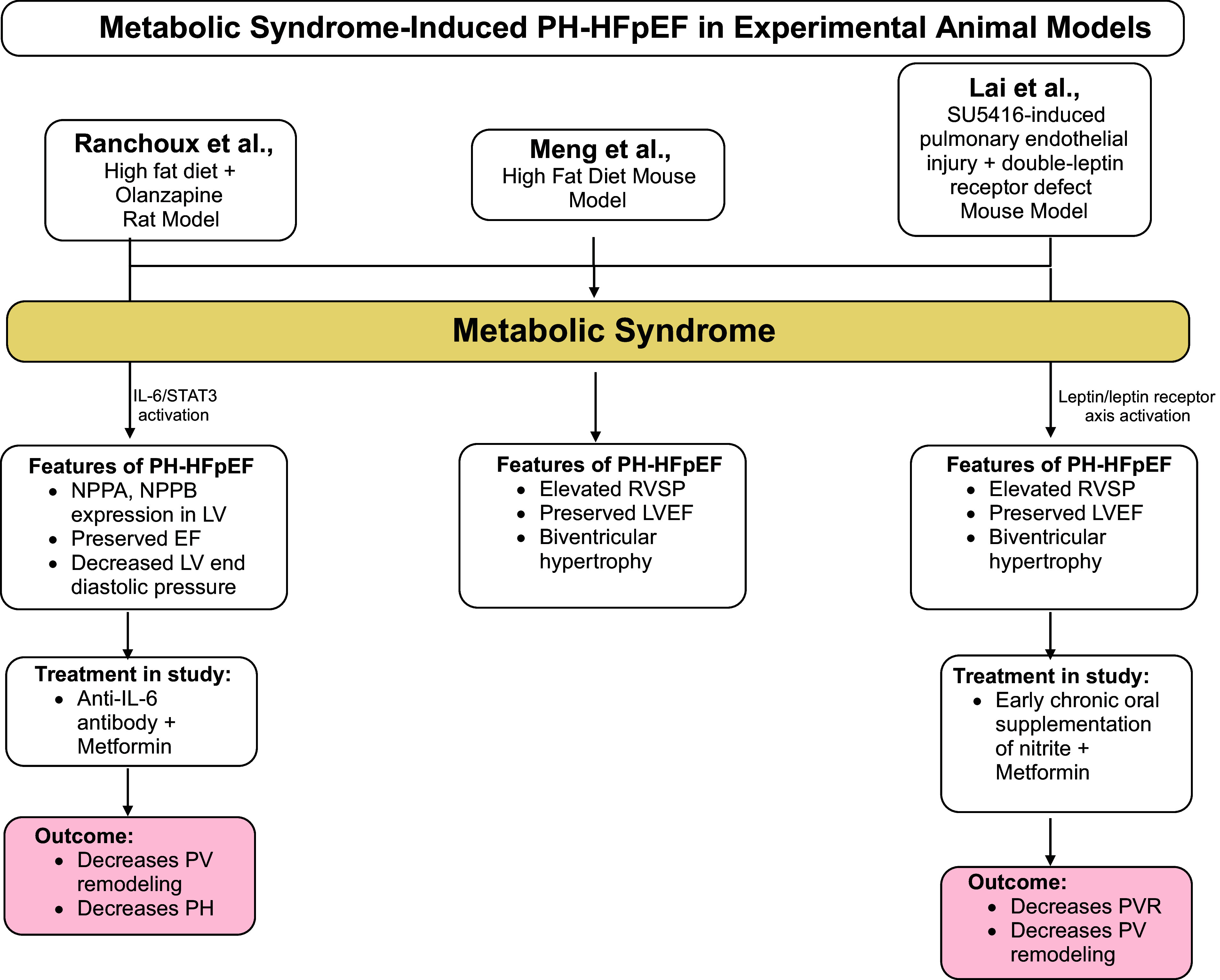
Heart failure (HF) with preserved ejection fraction (HFpEF) is the most common cause of pulmonary hypertension (PH) worldwide and is strongly associated with adverse clinical outcomes. The American Heart Association recently highlighted a call to action regarding the distinct lack of evidence-based treatments for PH due to poorly understood pathophysiology of PH attributable to HFpEF (PH-HFpEF). Prior studies have described cardiophysiological mechanisms to explain the development of isolated postcapillary PH (ipc-PH); however, the consequent increase in pulmonary vascular (PV) resistance (PVR) may lead to the less understood and more fatal combined pre- and postcapillary PH (cpc-PH). Metabolic disease and inflammatory dysregulation have been suggested to predispose PH, yet the molecular mechanisms are unknown. Although PH-HFpEF has been studied to partly share vasoactive neurohormonal mediators with primary pulmonary arterial hypertension (PAH), clinical trials that have targeted these pathways have been unsuccessful. The increased mortality of patients with PH-HFpEF necessitates further study into viable mechanistic targets involved in disease progression. We aim to summarize the current pathophysiological and clinical understanding of PH-HFpEF, highlight the role of known molecular mechanisms in the progression of PV disease, and introduce a novel concept that lipid metabolism may be attenuating and propagating PH-HFpEF. Our review addresses pulmonary hypertension (PH) attributable to heart failure (HF) with preserved ejection fraction (HFpEF; PH-HFpEF). Current knowledge gaps in PH-HFpEF pathophysiology have led to a lack of therapeutic targets. Thus, we address identified knowledge gaps in a comprehensive review, focusing on current clinical epidemiology, known pathophysiology, and previously studied molecular mechanisms. We also introduce a comprehensive review of polyunsaturated fatty acid (PUFA) lipid inflammatory mediators in PH-HFpEF.
射血分数保留的心力衰竭(HFpEF)是全球肺动脉高压(PH)最常见的原因,与不良临床结局密切相关。美国心脏协会最近强调,需要采取行动,解决由于对 HFpEF 所致 PH(PH-HFpEF)病理生理学认识不足,导致缺乏循证治疗方法的问题。先前的研究已经描述了一些心生理学机制,用以解释孤立性毛细血管后 PH(ipc-PH)的发生发展;然而,随之而来的肺血管(PV)阻力(PVR)增加可能导致对更具致命性的、了解较少的毛细血管前和毛细血管后混合 PH(cpc-PH)的认识不足。代谢性疾病和炎症失调被认为易患 PH,但分子机制尚不清楚。尽管 PH-HFpEF 部分与原发性肺动脉高压(PAH)的血管活性神经激素介质共享,但针对这些途径的临床试验均未成功。PH-HFpEF 患者的死亡率较高,需要进一步研究疾病进展中涉及的可行机制靶点。我们旨在总结 PH-HFpEF 的当前病理生理学和临床认识,强调已知分子机制在 PV 疾病进展中的作用,并引入一个新概念,即脂代谢可能减轻和促进 PH-HFpEF。我们的综述涉及心力衰竭(HF)伴射血分数保留(HFpEF)所致的肺动脉高压(PH);HFpEF 所致 PH(PH-HFpEF)的病理生理学目前存在知识空白,导致治疗靶点缺乏。因此,我们在全面综述中针对已确定的知识空白进行了探讨,重点关注当前的临床流行病学、已知的病理生理学和以前研究过的分子机制。我们还对 PH-HFpEF 中的多不饱和脂肪酸(PUFA)脂质炎症介质进行了全面综述。