Salas Ariel A, Gunn Elizabeth, Carlo Waldemar A, Bell Edward F, Das Abhik, Josephson Cassandra D, Patel Ravi M, Tan Sylvia, Kirpalani Haresh
Department of Pediatrics, University of Alabama at Birmingham.
Department of Pediatrics, University of Iowa, Iowa City.
JAMA Netw Open. 2024 May 1;7(5):e249643. doi: 10.1001/jamanetworkopen.2024.9643.
Observational studies often report that anemia and red blood cell (RBC) transfusions are associated with a higher risk of necrotizing enterocolitis (NEC) among extremely low-birthweight (ELBW) infants.
To evaluate whether there is a temporal association between 72-hour hazard periods of exposure to RBC transfusions and NEC among ELBW infants randomized to either higher or lower hemoglobin transfusion thresholds.
DESIGN, SETTING, AND PARTICIPANTS: This post hoc secondary analysis of 1690 ELBW infants who survived to postnatal day 10 enrolled in the Transfusion of Prematures (TOP) randomized multicenter trial between December 1, 2012, and April 12, 2017, was performed between June 2021 and July 2023.
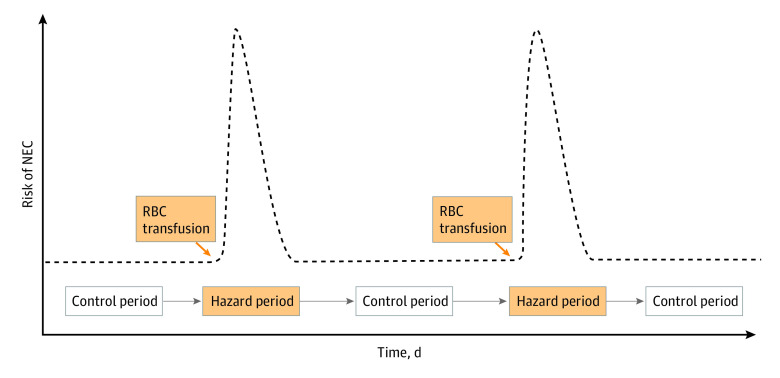
First, the distribution of RBC transfusions and the occurrence of NEC up to postnatal day 60 were examined. Second, 72-hour posttransfusion periods were categorized as hazard periods and the pretransfusion periods of variable duration as control periods. Then, the risk of NEC in posttransfusion hazard periods was compared with that in pretransfusion control periods, stratifying the risk based on randomization group (higher or lower hemoglobin transfusion threshold group).
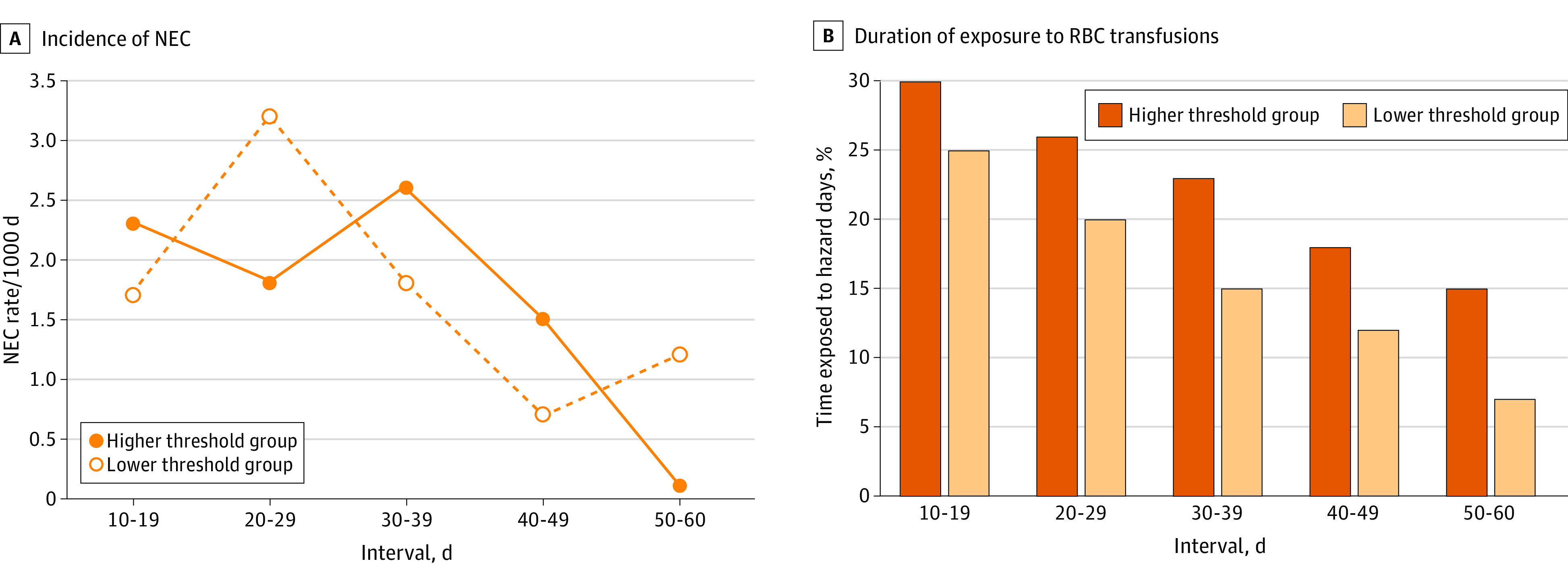
The primary outcome was incidence of NEC stage 2 or 3. Secondary outcomes included the incidence rates of NEC within five 10-day intervals, taking into account the number of days at risk.
Of 1824 ELBW infants randomized during the TOP trial, 1690 were included in the present analysis (mean [SD] gestational age, 26.0 [1.5] weeks; 899 infants [53.2%] were female). After categorizing 4947 hazard periods and 5813 control periods, we identified 133 NEC cases. Fifty-nine of these cases (44.4%) occurred during hazard periods. Baseline and clinical characteristics of infants with NEC during hazard periods did not differ from those of infants with NEC during control periods. The risk of NEC was 11.9 per 1000 posttransfusion hazard periods and 12.7 per 1000 control periods (adjusted risk ratio, 0.95; 95% CI, 0.68-1.32; P = .74). This risk did not differ significantly between randomization groups, but the incidence rate of NEC per 1000 days peaked between postnatal days 20 and 29 in the lower hemoglobin transfusion threshold group.
The findings of this post hoc analysis suggest that, among ELBW infants with the hemoglobin ranges occurring in the TOP trial, exposure to RBC transfusions was not temporally associated with a higher risk of NEC during 72-hour posttransfusion hazard periods. Given that the incidence rate of NEC peaked between postnatal days 20 and 29 among infants with lower hemoglobin values, a more in-depth examination of this at-risk period using larger data sets is warranted.
ClinicalTrials.gov Identifier: NCT01702805.
观察性研究经常报告,贫血和红细胞(RBC)输血与极低出生体重(ELBW)婴儿发生坏死性小肠结肠炎(NEC)的较高风险相关。
评估随机分配到较高或较低血红蛋白输血阈值的ELBW婴儿中,红细胞输血暴露的72小时危险时段与坏死性小肠结肠炎之间是否存在时间关联。
设计、背景和参与者:这项事后二次分析纳入了1690名出生后存活至第10天的ELBW婴儿,这些婴儿参加了2012年12月1日至2017年4月12日期间的早产输血(TOP)随机多中心试验,分析于2021年6月至2023年7月进行。
首先,检查出生后60天内红细胞输血的分布情况和坏死性小肠结肠炎的发生情况。其次,将输血后72小时时段分类为危险时段,将不同持续时间的输血前时段作为对照时段。然后,比较输血后危险时段坏死性小肠结肠炎的风险与输血前对照时段的风险,并根据随机分组(较高或较低血红蛋白输血阈值组)对风险进行分层。
主要结局是2期或3期坏死性小肠结肠炎的发病率。次要结局包括在五个10天间隔内坏死性小肠结肠炎的发病率,并考虑到风险天数。
在TOP试验中随机分组的1824名ELBW婴儿中,1690名纳入本分析(平均[标准差]胎龄,26.0[1.5]周;899名婴儿[53.2%]为女性)。在将4947个危险时段和5813个对照时段分类后,我们确定了133例坏死性小肠结肠炎病例。其中59例(44.4%)发生在危险时段。危险时段发生坏死性小肠结肠炎的婴儿的基线和临床特征与对照时段发生坏死性小肠结肠炎的婴儿无差异。每1000个输血后危险时段坏死性小肠结肠炎的风险为11.9,每1000个对照时段为12.7(调整风险比,0.95;95%置信区间,0.68 - 1.32;P = 0.74)。随机分组之间的这种风险无显著差异,但较低血红蛋白输血阈值组每1000天坏死性小肠结肠炎的发病率在出生后第20天至第29天达到峰值。
这项事后分析的结果表明,在TOP试验中血红蛋白范围内的ELBW婴儿中,输血后72小时危险时段内红细胞输血暴露与坏死性小肠结肠炎的较高风险无时间关联。鉴于血红蛋白值较低的婴儿中坏死性小肠结肠炎的发病率在出生后第20天至第(此处原文有误,应为29天)29天达到峰值,有必要使用更大的数据集对这一风险期进行更深入的研究。
ClinicalTrials.gov标识符:NCT01702805。