Cardiometabolic Center, Fuwai Hospital, National Center for Cardiovascular Diseases, Chinese Academy of Medical Sciences & Peking Union Medical College, Beijing, 100037, China.
Lipids Health Dis. 2024 May 7;23(1):134. doi: 10.1186/s12944-024-02078-0.
Remnant cholesterol (RC) and nonhigh-density lipoprotein cholesterol (nonHDL-C) are key risk factors for atherosclerotic cardiovascular disease (ASCVD), with apolipoprotein B (apoB) and lipoprotein(a) [Lp(a)] also contributing to its residual risk. However, real-world population-based evidence regarding the impact of current clinical LDL-C-centric lipid-lowering therapy (LLT) on achieving RC and nonHDL-C goals, as well as on modifying residual CVD risk factors is limited.
This prospective observational study enrolled 897 CVD patients from September, 2020 to July, 2021. All participants had previously received low-/moderate-intensity LLT and were discharged with either low-/moderate-intensity LLT or high-intensity LLT. After a median follow-up of 3 months, changes in RC, nonHDL-C, and other biomarkers were assessed. Multivariate logistic regression was performed to analyze the impact of the LLT on goal attainment.
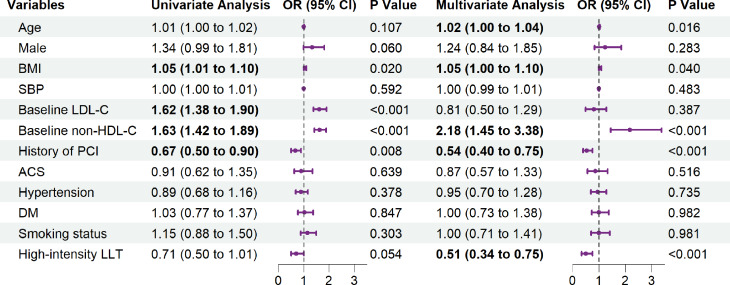
Among all patients, 83.50% transitioned to high-intensity LLT from low or moderate. After follow-up, the high-intensity group saw significantly greater reductions in RC (-20.51% vs. -3.90%, P = 0.025), nonHDL-C (-25.12% vs. 0.00%, P < 0.001), apoB (-19.35% vs. -3.17%, P < 0.001), triglycerides (-17.82% vs. -6.62%, P < 0.001), and LDL-C and total cholesterol. Spearman correlation analysis revealed that LDL-C reduction from current LLT was strongly correlated with nonHDL-C reduction (r = 0.87, P < 0.001). Patients who received high-intensity LLT had significant improvements in attainment of RC (from 44.2% to 60.7%, χ² = 39.23, P < 0.001) and nonHDL-C (from 19.4% to 56.9%, χ² = 226.06, P < 0.001) goals. Furthermore, multivariate logistic regression showed that high-intensity LLT was a protective factor for RC [odds ratio (OR) = 0.66; 95% confidence intervals (CI), 0.45-0.97; P = 0.033] and nonHDL-C goal attainment (OR = 0.51; 95% CI, 0.34-0.75; P < 0.001), without a significant increase of adverse reactions.
Current levels of clinically prescribed LDL-C-centric treatment can reduce RC and other lipid-related residual risk factors, but high-intensity LLT is better at achieving nonHDL-C and RC goals than low-/moderate-intensity LLT, with a good safety profile. More targeted RC treatments are still needed to reduce residual lipid risk further.
残余胆固醇(RC)和非高密度脂蛋白胆固醇(nonHDL-C)是动脉粥样硬化性心血管疾病(ASCVD)的关键风险因素,载脂蛋白 B(apoB)和脂蛋白(a)[Lp(a)]也有助于其残余风险。然而,目前基于人群的关于当前临床 LDL-C 为中心的降脂治疗(LLT)对实现 RC 和 nonHDL-C 目标的影响,以及对改善残余 CVD 风险因素的影响的实际证据有限。
这项前瞻性观察研究纳入了 2020 年 9 月至 2021 年 7 月期间的 897 例 CVD 患者。所有患者均接受过低/中强度 LLT,并接受低/中强度 LLT 或高强度 LLT 出院。中位随访 3 个月后,评估 RC、nonHDL-C 和其他生物标志物的变化。采用多变量逻辑回归分析 LLT 对目标实现的影响。
在所有患者中,83.50%从低或中强度过渡到高强度 LLT。随访后,高强度组的 RC(-20.51%比-3.90%,P=0.025)、nonHDL-C(-25.12%比 0.00%,P<0.001)、apoB(-19.35%比-3.17%,P<0.001)、甘油三酯(-17.82%比-6.62%,P<0.001)和 LDL-C 和总胆固醇的降幅明显更大。Spearman 相关分析显示,当前 LLT 降低 LDL-C 与降低 nonHDL-C 呈强相关(r=0.87,P<0.001)。接受高强度 LLT 的患者在实现 RC(从 44.2%到 60.7%,χ²=39.23,P<0.001)和 nonHDL-C(从 19.4%到 56.9%,χ²=226.06,P<0.001)目标方面有显著改善。此外,多变量逻辑回归显示,高强度 LLT 是 RC[比值比(OR)=0.66;95%置信区间(CI),0.45-0.97;P=0.033]和 nonHDL-C 目标实现(OR=0.51;95%CI,0.34-0.75;P<0.001)的保护因素,且不良反应无显著增加。
目前临床规定的 LDL-C 为中心的治疗可以降低 RC 和其他与脂质相关的残余风险因素,但高强度 LLT 比低/中强度 LLT 更能实现 nonHDL-C 和 RC 目标,且安全性良好。仍需要更有针对性的 RC 治疗来进一步降低残余脂质风险。