Navuluri Neelima, Kussin Peter S, Egger Joseph R, Birgen Elcy, Kitur Sylvia, Thielman Nathan M, Parish Alice, Green Cynthia L, Janko Mark M, Diero Lameck, Wools-Kaloustian Kara, Lagat David, Que Loretta G
Department of Medicine.
Duke Global Health Institute, Duke University, Durham, North Carolina.
Ann Am Thorac Soc. 2024 Aug;21(8):1176-1185. doi: 10.1513/AnnalsATS.202402-167OC.
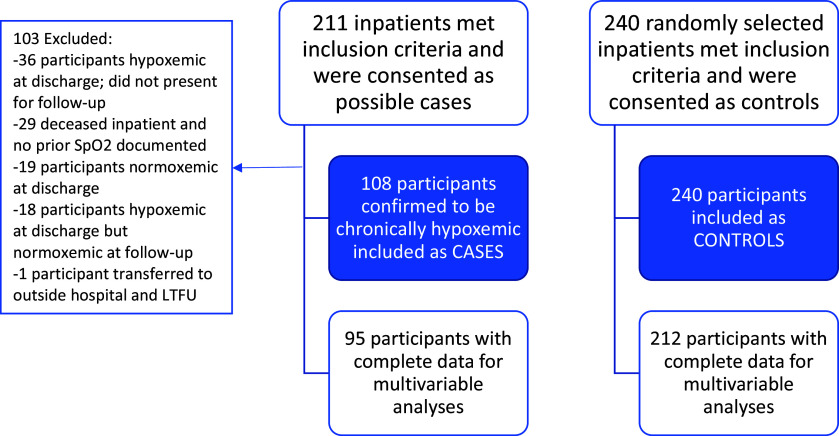
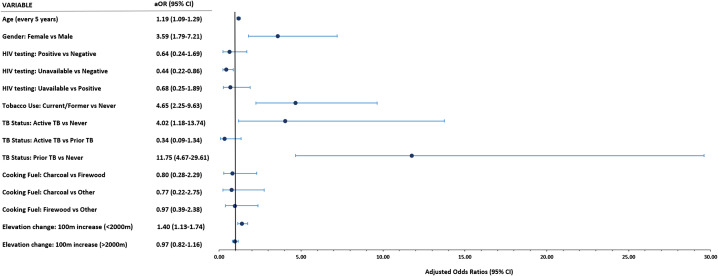
Data on risk factors for chronic hypoxemia in low- and middle-income countries are lacking. We aimed to quantify the association between potential risk factors and chronic hypoxemia among adults hospitalized in Kenya. A hospital-based, case-control study was conducted at Moi Teaching and Referral Hospital in Eldoret, Kenya. Adult inpatients were screened on admission and enrolled in a 1:2 case-to-control ratio. Cases were patients with chronic hypoxemia, defined as resting oxygen saturation as measured by pulse oximetry (Sp) ⩽ 88% on admission and either 1-month postdischarge Sp ⩽ 88% or, if they died before follow-up, documented Sp ⩽ 88% in the 6 months before enrollment. Control subjects were randomly selected, stratified by sex, among nonhypoxemic inpatients. Data were collected using questionnaires and structured chart review. Regression was used to assess the associations between chronic hypoxemia and age, sex, smoking status, biomass fuel use, elevation, and self-reported history of tuberculosis and human immunodeficiency virus diagnosis. Odds ratios (ORs) and 95% confidence intervals (CIs) are reported. We enrolled 108 chronically hypoxemic cases and 240 nonhypoxemic control subjects into our Chronic Hypoxemia among Kenyan Adults (CHAKA) cohort. In multivariable analysis, compared with control subjects, chronically hypoxemic cases had significantly higher odds of older age (OR, 1.2 per 5-year increase [95% CI, 1.1-1.3]), female sex (OR, 3.6 [95% CI, 1.8-7.2]), current or former tobacco use (OR, 4.7 [95% CI, 2.3-9.6]), and prior tuberculosis (OR, 11.8 [95% CI, 4.7-29.6]) but no increase in the odds of human immunodeficiency virus diagnosis and biomass fuel use. These findings highlight the potential impact of prior tuberculosis on chronic lung disease in Kenya and the need for further studies on posttuberculosis lung disease.
低收入和中等收入国家中慢性低氧血症风险因素的数据匮乏。我们旨在量化肯尼亚住院成人中潜在风险因素与慢性低氧血症之间的关联。在肯尼亚埃尔多雷特的莫伊教学与转诊医院开展了一项基于医院的病例对照研究。成年住院患者在入院时接受筛查,并按照1:2的病例对照比例入组。病例为慢性低氧血症患者,定义为入院时经脉搏血氧饱和度仪测量的静息氧饱和度(Sp)≤88%,且出院后1个月Sp≤88%,或者如果在随访前死亡,则在入组前6个月记录的Sp≤88%。对照对象在非低氧血症住院患者中按性别分层随机选取。通过问卷调查和结构化病历审查收集数据。采用回归分析评估慢性低氧血症与年龄、性别、吸烟状况、生物质燃料使用、海拔以及自我报告的结核病和人类免疫缺陷病毒诊断史之间的关联。报告了比值比(OR)和95%置信区间(CI)。我们将108例慢性低氧血症病例和240例非低氧血症对照对象纳入了我们的肯尼亚成人慢性低氧血症(CHAKA)队列。在多变量分析中,与对照对象相比,慢性低氧血症病例在年龄较大(每增加5岁OR为1.2 [95% CI,1.1 - 1.3])、女性(OR为3.6 [95% CI,1.8 - 7.2])、当前或既往吸烟(OR为4.7 [95% CI,2.3 - 9.6])以及既往结核病(OR为11.8 [95% CI,4.7 - 29.6])方面的比值显著更高,但人类免疫缺陷病毒诊断和生物质燃料使用的比值没有增加。这些发现凸显了既往结核病对肯尼亚慢性肺病的潜在影响以及对结核病后肺病进行进一步研究的必要性。