Department of Anesthesiology, Chaohu Hospital of Anhui Medical University, Chaohu, Anhui, China (mainland).
Med Sci Monit. 2024 May 20;30:e944022. doi: 10.12659/MSM.944022.
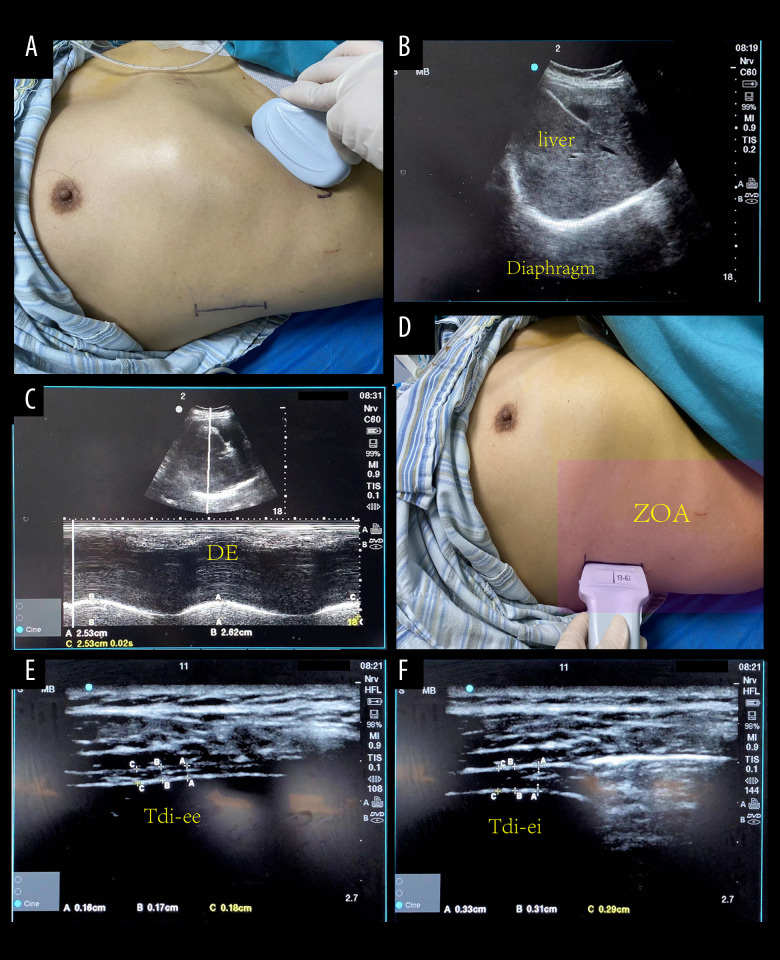
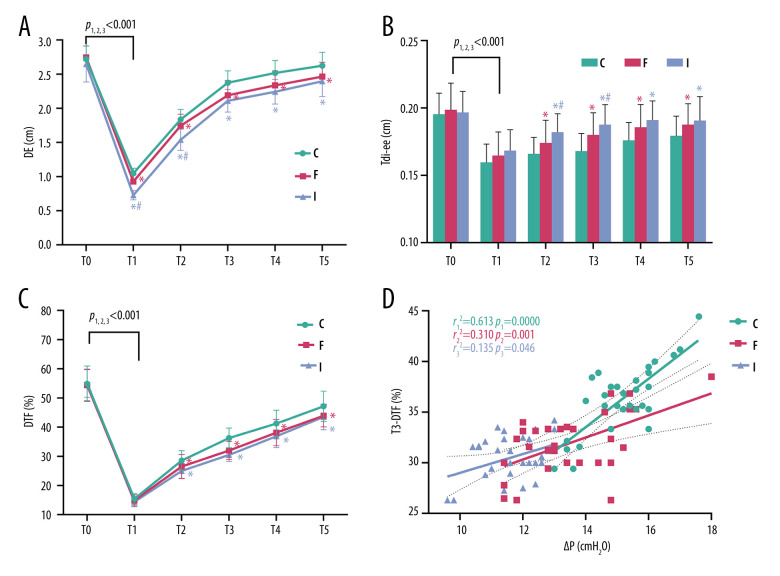
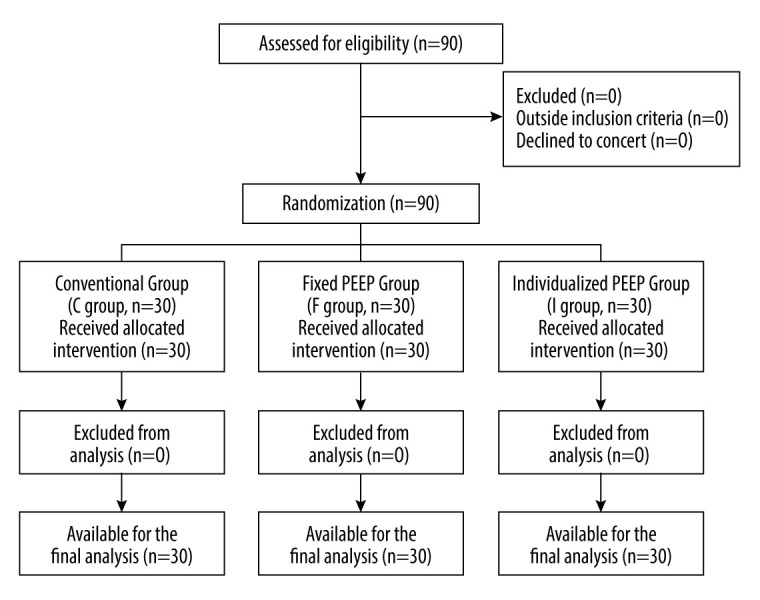
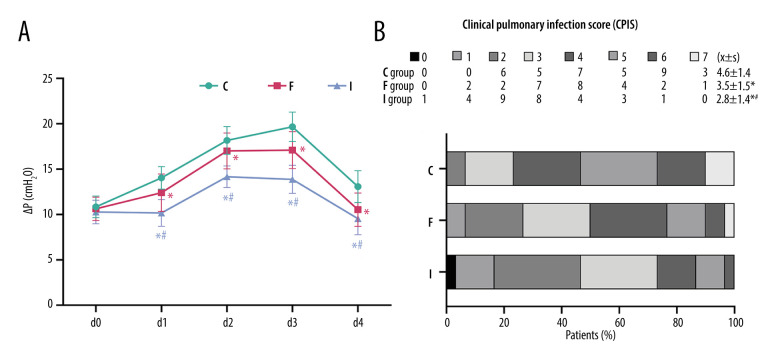
BACKGROUND The concept of driving pressure (ΔP) has been established to optimize mechanical ventilation-induced lung injury. However, little is known about the specific effects of setting individualized positive end-expiratory pressure (PEEP) with driving pressure guidance on patient diaphragm function. MATERIAL AND METHODS Ninety patients were randomized into 3 groups, with PEEP set to 0 in group C; 5 cmH₂O in group F; and individualized PEEP in group I, based on esophageal manometry. Diaphragm ultrasound was performed in the supine position at 6 consecutive time points from T0-T5: diaphragm excursion, end-expiratory diaphragm thickness (Tdi-ee), and diaphragm thickening fraction (DTF) were measured. Primary indicators included diaphragm excursion, Tdi-ee, and DTF at T0-T5, and the correlation between postoperative DTF and ΔP. Secondary indicators included respiratory mechanics, hemodynamic changes at intraoperative d0-d4 time points, and postoperative clinical pulmonary infection scores. RESULTS (1) Diaphragm function parameters reached the lowest point at T1 in all groups (P<0.001). (2) Compared with group C, diaphragm excursion decreased, Tdi-ee increased, and DTF was lower in groups I and F at T1-T5, with significant differences (P<0.05), but the differences between groups I and F were not significant (P>0.05). (3) DTF was significantly and positively correlated with mean intraoperative ΔP in each group at T3, and the correlation was stronger at higher levels of ΔP. CONCLUSIONS Individualized PEEP, achieved by esophageal manometry, minimizes diaphragmatic injury caused by mechanical ventilation based on lung protection, but its protection of the diaphragm during laparoscopic surgery is not superior to that of conventional ventilation strategies.
驱动压(ΔP)的概念已经确立,以优化机械通气引起的肺损伤。然而,对于设定个体化呼气末正压(PEEP)以指导驱动压对患者膈肌功能的具体影响知之甚少。
90 名患者随机分为 3 组,C 组 PEEP 设置为 0;F 组为 5cmH₂O;I 组根据食管测压法设置个体化 PEEP。膈肌超声在仰卧位进行,从 T0 到 T5 连续 6 个时间点:测量膈肌位移、呼气末膈肌厚度(Tdi-ee)和膈肌增厚分数(DTF)。主要指标包括 T0-T5 时的膈肌位移、Tdi-ee 和 DTF,以及术后 DTF 与ΔP 的相关性。次要指标包括术中 d0-d4 时间点的呼吸力学、血流动力学变化和术后临床肺部感染评分。
(1)所有组的膈肌功能参数在 T1 时均达到最低点(P<0.001)。(2)与 C 组相比,I 组和 F 组在 T1-T5 时的膈肌位移减小,Tdi-ee 增加,DTF 降低,差异有统计学意义(P<0.05),但 I 组和 F 组之间的差异无统计学意义(P>0.05)。(3)在每组中,DTF 与术中平均ΔP 在 T3 时呈显著正相关,且在较高的ΔP 水平时相关性更强。
通过食管测压法实现的个体化 PEEP,基于肺保护最大限度地减少机械通气引起的膈肌损伤,但在腹腔镜手术中对膈肌的保护并不优于常规通气策略。