Abber Sophie R, Becker Kendra R, Stern Casey M, Palmer Lilian P, Joiner Thomas E, Breithaupt Lauren, Kambanis Paraskevi Evelyna, Eddy Kamryn T, Thomas Jennifer J, Burton-Murray Helen
Department of Psychology, Florida State University, Tallahassee, FL, USA.
Eating Disorders Clinical and Research Program, Department of Psychiatry, Massachusetts General Hospital, Boston, MA, USA.
Psychol Med. 2024 Aug;54(11):2956-2966. doi: 10.1017/S003329172400103X. Epub 2024 May 27.
differentiates avoidant/restrictive food intake disorder (ARFID) from other eating disorders (EDs) by a lack of overvaluation of body weight/shape driving restrictive eating. However, clinical observations and research demonstrate ARFID and shape/weight motivations sometimes co-occur. To inform classification, we: (1) derived profiles underlying restriction motivation and examined their validity and (2) described diagnostic characterizations of individuals in each profile to explore whether findings support current diagnostic schemes. We expected, consistent with , that profiles would comprise individuals endorsing solely ARFID or restraint (i.e. trying to eat less to control shape/weight) motivations.
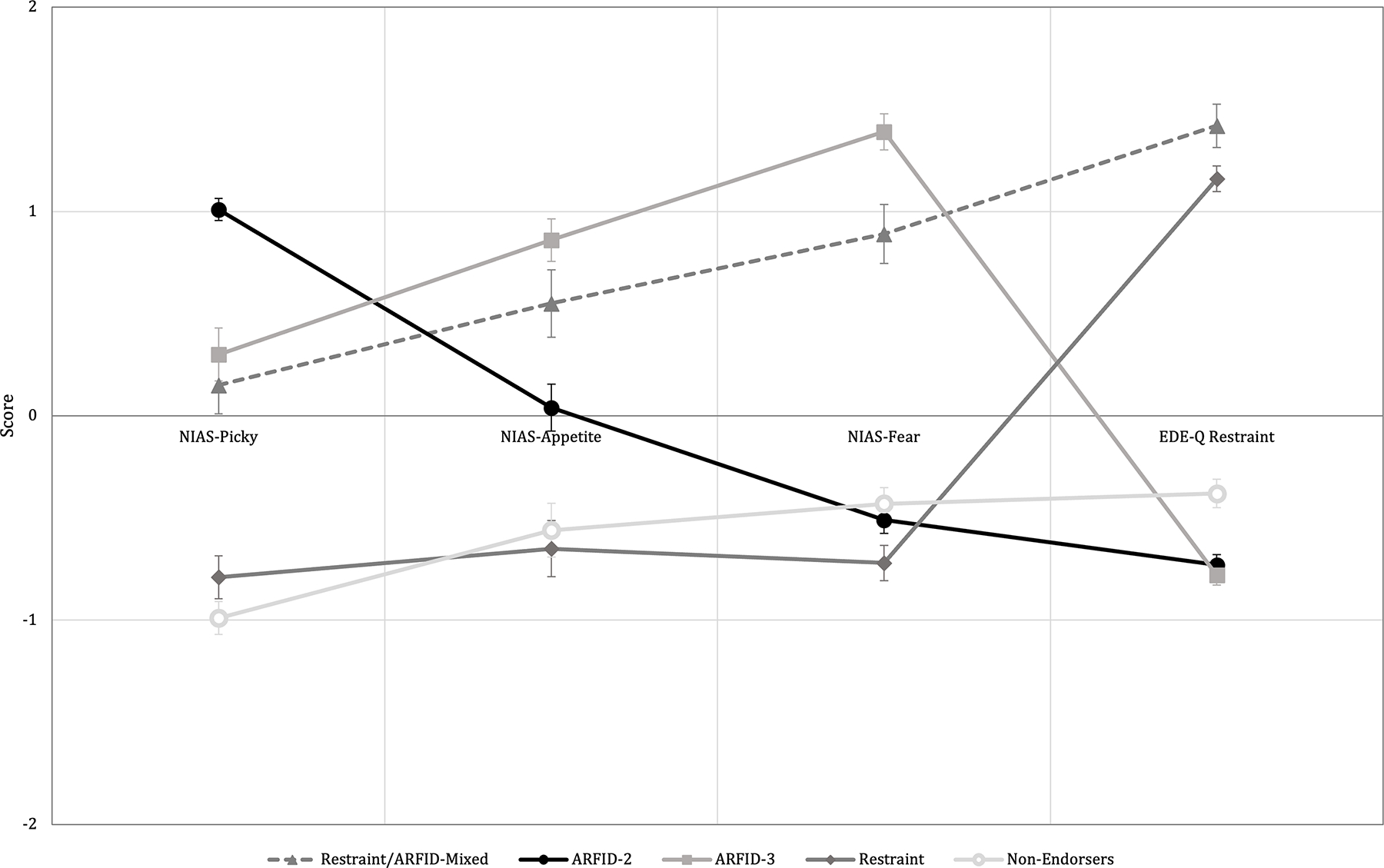
We applied latent profile analysis to 202 treatment-seeking individuals (ages 10-79 years [ = 26, s.d. = 14], 76% female) with ARFID or a non-ARFID ED, using the Nine-Item ARFID Screen (Picky, Appetite, and Fear subscales) and the Eating Disorder Examination-Questionnaire Restraint subscale as indicators.
A 5-profile solution emerged: Restraint/ARFID-Mixed ( = 24; 8% [ = 2] with ARFID diagnosis); ARFID-2 (with Picky/Appetite; = 56; 82% ARFID); ARFID-3 (with Picky/Appetite/Fear; = 40; 68% ARFID); Restraint ( = 45; 11% ARFID); and Non-Endorsers ( = 37; 2% ARFID). Two profiles comprised individuals endorsing solely ARFID motivations (ARFID-2, ARFID-3) and one comprising solely restraint motivations (Restraint), consistent with . However, Restraint/ARFID-Mixed (92% non-ARFID ED diagnoses, comprising 18% of those with non-ARFID ED diagnoses in the full sample) endorsed ARFID restraint motivations.
The heterogeneous profiles identified suggest ARFID and restraint motivations for dietary restriction may overlap somewhat and that individuals with non-ARFID EDs can also endorse high ARFID symptoms. Future research should clarify diagnostic boundaries between ARFID and non-ARFID EDs.
回避/限制型食物摄入障碍(ARFID)与其他饮食失调(EDs)的区别在于,其限制饮食并非由对体重/体型的过度重视所驱动。然而,临床观察和研究表明,ARFID与体型/体重动机有时会同时出现。为了为分类提供依据,我们:(1)推导了限制动机背后的概况,并检验了其有效性;(2)描述了每个概况中个体的诊断特征,以探讨研究结果是否支持当前的诊断方案。我们预期,与[未提及的相关内容]一致,这些概况将包括仅认可ARFID或节制(即试图少吃以控制体型/体重)动机的个体。
我们对202名寻求治疗的个体(年龄10 - 79岁[均值 = 26,标准差 = 14],76%为女性)进行了潜在概况分析,这些个体患有ARFID或非ARFID型饮食失调,使用九项ARFID筛查量表(挑食、食欲和恐惧分量表)以及饮食失调检查问卷的节制分量表作为指标。
出现了一个五概况解决方案:节制/ARFID混合型(n = 24;8%[n = 2]患有ARFID诊断);ARFID - 2型(伴有挑食/食欲;n = 56;82%为ARFID);ARFID - 3型(伴有挑食/食欲/恐惧;n = 40;68%为ARFID);节制型(n = 45;11%为ARFID);以及非认可型(n = 37;2%为ARFID)。与[未提及的相关内容]一致,有两个概况包括仅认可ARFID动机的个体(ARFID - 2型,ARFID - 3型),一个包括仅认可节制动机的个体(节制型)。然而,节制/ARFID混合型(92%为非ARFID型饮食失调诊断,占全样本中非ARFID型饮食失调诊断个体的18%)认可ARFID和节制动机。
所确定的异质概况表明,ARFID和饮食限制的节制动机可能在一定程度上重叠,并且非ARFID型饮食失调的个体也可能认可较高的ARFID症状。未来的研究应明确ARFID与非ARFID型饮食失调之间的诊断界限。