Pereira Eduardo Maia Martins, Nascimento Tatiana Souza do, da Costa Mariana Gaya, Slawka Eric, Júnior Carlos Galhardo
Universidade Federal de Minas Gerais, Departamento de Medicina, Belo Horizonte, MG, Brazil.
Hospital Federal Cardoso Fontes, Departamento de Anestesiologia, Rio de Janeiro, RJ, Brazil.
Braz J Anesthesiol. 2024 Sep-Oct;74(5):844520. doi: 10.1016/j.bjane.2024.844520. Epub 2024 May 25.
Midazolam is routinely used as preanesthetic medication in pediatric patients. Recently, dexmedetomidine has emerged as an alternative as a premedicant. We aimed to add more evidence about the efficacy and safety of two common routes of administration for pediatric premedication: oral midazolam versus intranasal dexmedetomidine.
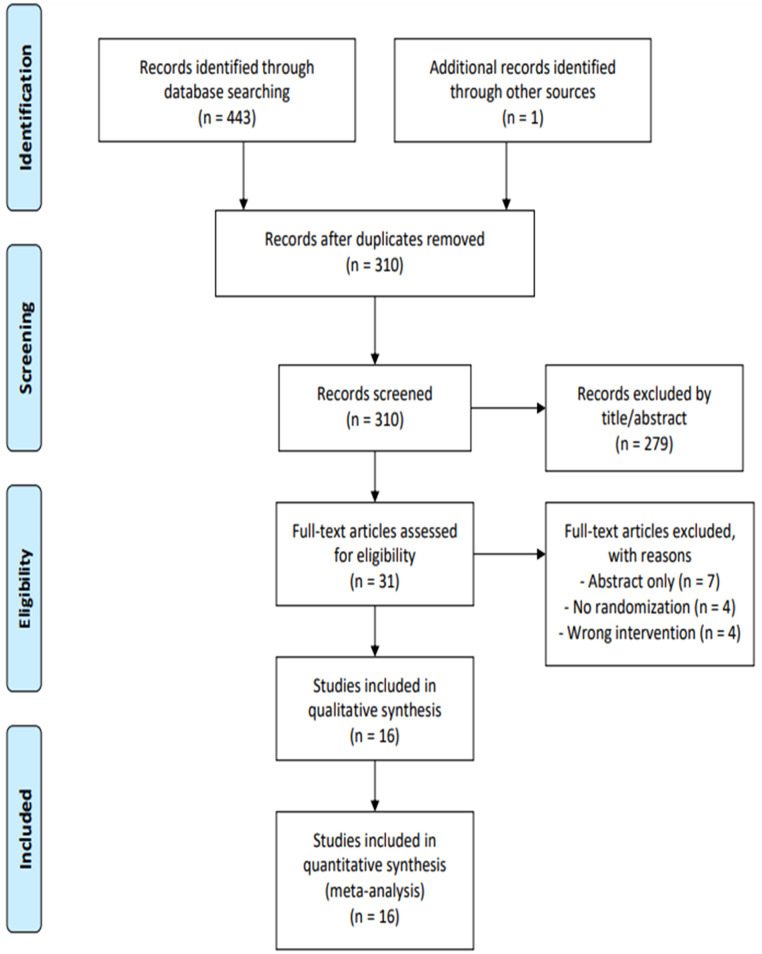
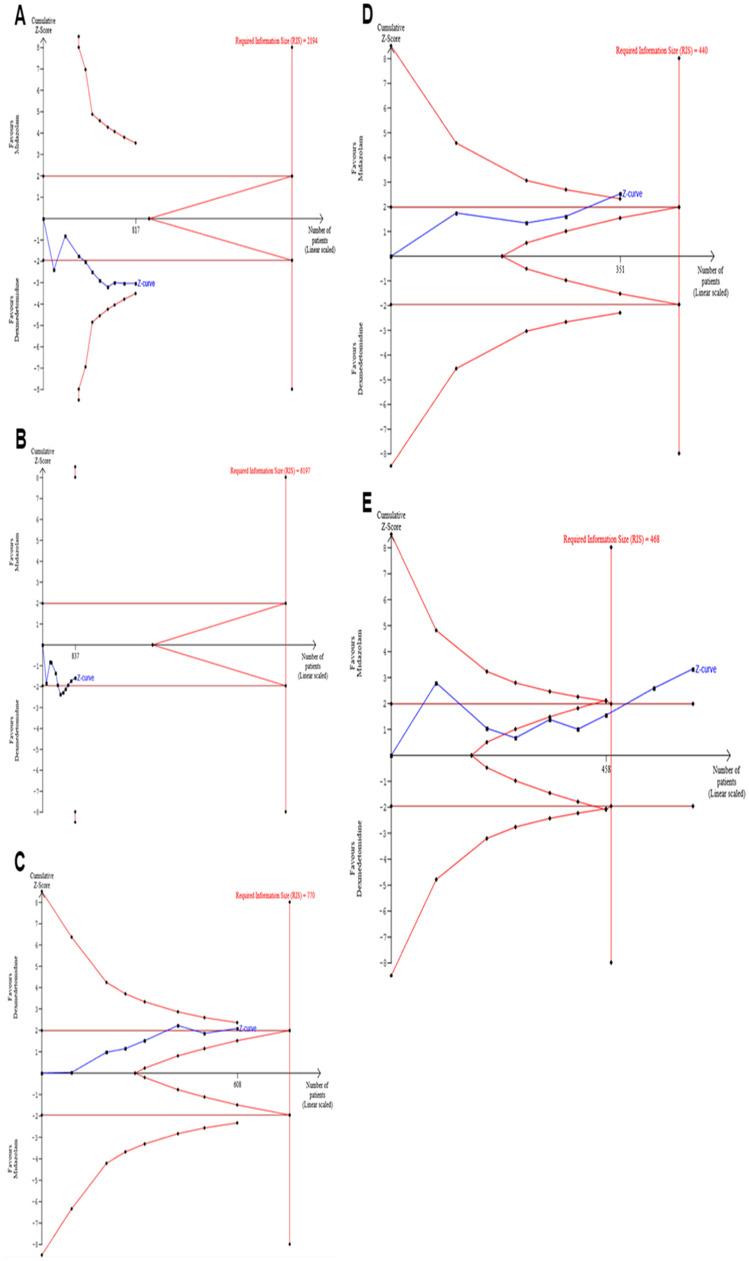
We systematically searched Randomized Controlled Trials (RCTs) involving patients ≤ 18 years old undergoing preanesthetic medication and comparing intranasal dexmedetomidine with oral midazolam. Risk Ratio (RR) and Mean Difference (MD) with 95% Confidence Intervals (95% CI) were computed using a random effects model. Trial-sequential analyses were performed to assess inconsistency.
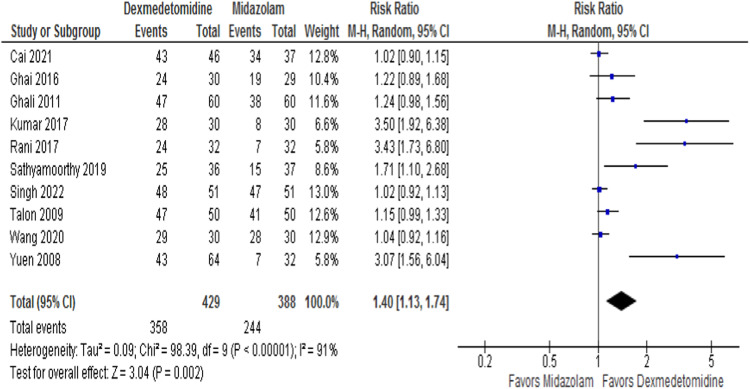
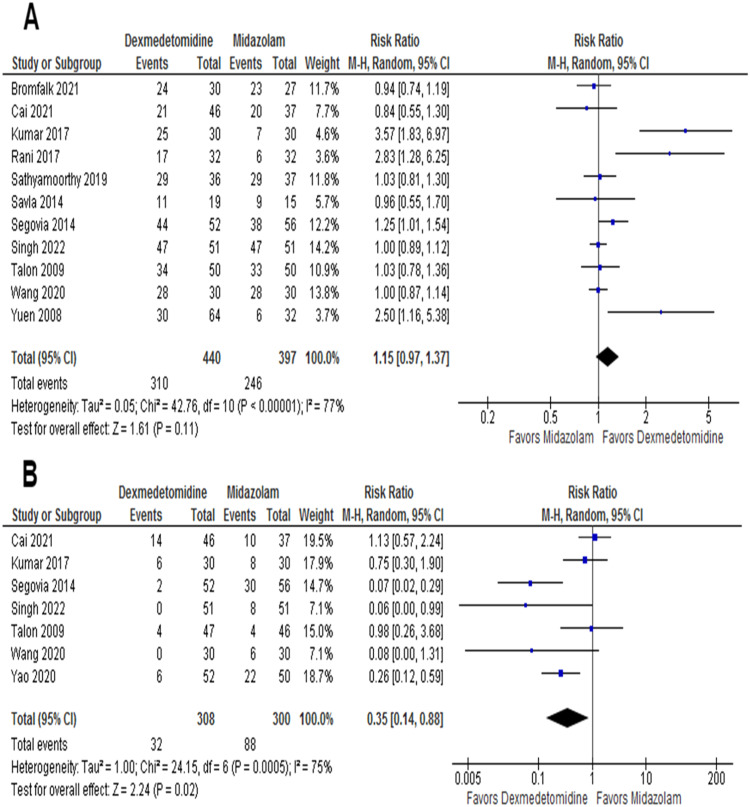
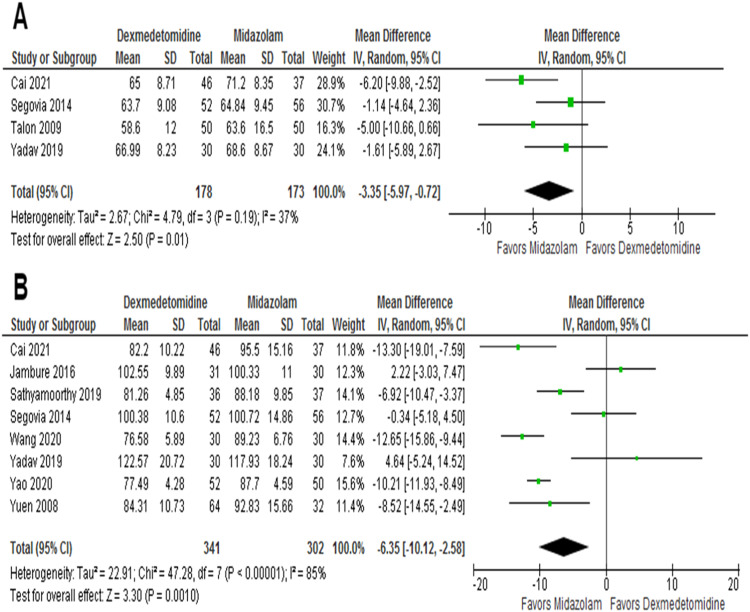
Sixteen RCTs (1,239 patients) were included. Mean age was 5.5 years old, and most procedures were elective. There was no difference in satisfactory induction or mask acceptance (RR = 1.15, 95% CI 0.97-1.37; p = 0.11). There was a higher incidence of satisfactory separation from parents in the dexmedetomidine group (RR = 1.40; 95% CI 1.13-1.74; p = 0.002). Dexmedetomidine was also associated with a reduction in the incidence of emergence agitation (RR = 0.35; 95% CI 0.14-0.88; p = 0.02). Heart rate and mean arterial pressure were marginally lower in the dexmedetomidine group but without clinical repercussions.
Compared with oral midazolam, intranasal dexmedetomidine demonstrated better separation from parents and lower incidence of emergence agitation in pediatric premedication, without a difference in satisfactory induction. Intranasal dexmedetomidine may be a safe and effective alternative to oral midazolam for premedication in pediatric patients.
咪达唑仑常用于小儿患者的麻醉前用药。近年来,右美托咪定已成为一种替代的术前用药。我们旨在补充更多关于小儿术前用药两种常见给药途径(口服咪达唑仑与鼻内给予右美托咪定)的疗效和安全性的证据。
我们系统检索了涉及18岁及以下接受麻醉前用药患者且比较鼻内给予右美托咪定与口服咪达唑仑的随机对照试验(RCT)。采用随机效应模型计算风险比(RR)和平均差(MD)以及95%置信区间(95%CI)。进行序贯分析以评估不一致性。
纳入了16项RCT(1239例患者)。平均年龄为5.5岁,大多数手术为择期手术。在诱导满意或面罩接受方面无差异(RR = 1.15,95%CI 0.97 - 1.37;p = 0.11)。右美托咪定组与父母顺利分离的发生率更高(RR = 1.40;95%CI 1.13 - 1.74;p = 0.002)。右美托咪定还与苏醒期躁动发生率降低相关(RR = 0.35;95%CI 0.14 - 0.88;p = 0.02)。右美托咪定组的心率和平均动脉压略低,但无临床影响。
与口服咪达唑仑相比,鼻内给予右美托咪定在小儿术前用药中显示出与父母更好的分离效果和更低的苏醒期躁动发生率,诱导满意程度无差异。鼻内给予右美托咪定可能是小儿患者术前用药中口服咪达唑仑的一种安全有效的替代方法。